Iron Tablets and Blood Pressure
You started taking iron supplements, and now your blood pressure readings look different. Coincidence or cause for concern? The short answer: can iron tablets increase blood pressure? For most healthy people, no. But the full picture is more complex than a simple yes or no.
Research indicates that iron supplementation does not typically raise blood pressure in individuals with normal cardiovascular function. However, people with pre-existing hypertension, those on blood pressure medications, or anyone taking high doses may experience measurable cardiovascular shifts. The relationship depends heavily on your baseline health, iron status, and dosage.
Iron tablets do not directly increase blood pressure in healthy individuals, but they may contribute to cardiovascular changes in people with hypertension, those using antihypertensive medications, or individuals prone to iron overload.
What Current Research Says
A large-scale prospective study using UK Biobank data from 427,939 participants found no significant association between habitual iron supplementation and adverse outcomes in normotensive individuals. Yet among hypertensive participants, iron supplement users showed a 12% higher risk of kidney-related complications, particularly those already taking blood pressure medication. Cross-sectional research has also linked elevated ferritin levels — a marker of iron stores — with increased hypertension risk. So does iron cause high blood pressure directly? The evidence points more toward iron amplifying existing cardiovascular vulnerabilities rather than creating new ones from scratch.
Why This Question Matters for Supplement Users
Iron is one of the most commonly used supplements worldwide, frequently prescribed for anemia and taken by millions without routine cardiovascular monitoring. If you have noticed a change in your readings and wondered whether iron supplements can cause high blood pressure, you are asking the right question. Does iron affect blood pressure? It can, under specific circumstances. Whether iron raises blood pressure in your case depends on factors like your current iron levels, supplement dosage, and cardiovascular history. The sections ahead break down exactly how iron interacts with your heart and blood vessels, which populations face the highest risk, and what you can do to stay safe while supplementing.
How Iron Interacts With Your Cardiovascular System
Understanding the link between iron and blood pressure starts with a basic question: what does iron actually do inside your blood vessels? Iron is not just a nutrient sitting passively in your body. It plays active roles in oxygen delivery, blood vessel dilation, and heart rate regulation — all of which feed directly into your blood pressure readings.
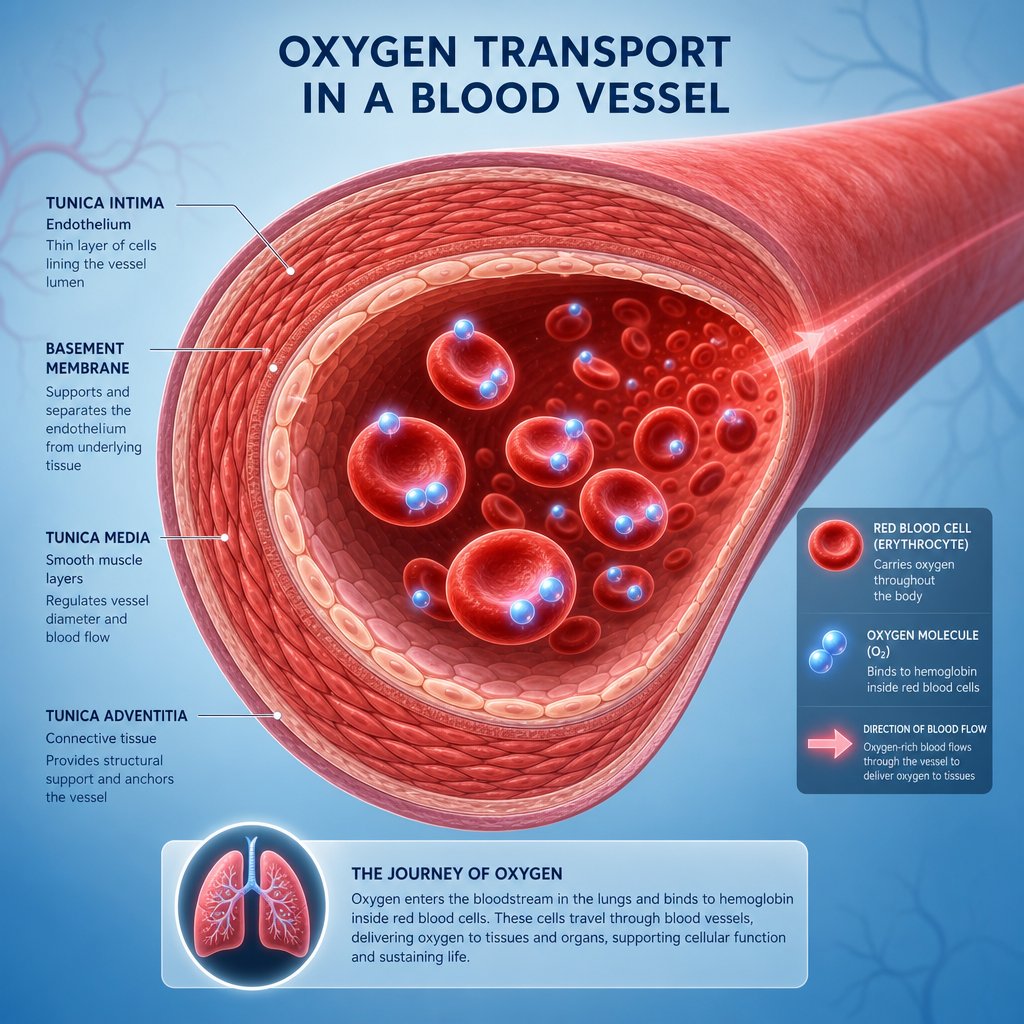
Iron and Oxygen Transport in Blood Vessels
Hemoglobin, the protein inside red blood cells responsible for carrying oxygen, depends on iron to function. Each hemoglobin molecule contains four iron-containing heme groups, and each one binds a single oxygen molecule. Roughly 98% of all oxygen in your blood travels bound to hemoglobin rather than dissolved freely in plasma.
When iron levels drop, your body produces less functional hemoglobin. Fewer oxygen molecules reach your tissues, and your cardiovascular system compensates. Heart rate increases. Blood vessels adjust their tone. These compensatory shifts directly influence blood pressure and iron status becomes a hidden variable in your readings.
Conversely, when iron stores are adequate and hemoglobin levels normalize, oxygen delivery stabilizes, and the heart no longer needs to work overtime. This is why iron deficiency and blood pressure are so closely intertwined — not because iron acts on blood vessels like a drug, but because it determines how efficiently your circulatory system operates.
The Role of Nitric Oxide and Vascular Tone
Here is where things get more nuanced. Nitric oxide (NO) is a signaling molecule your blood vessels produce to relax and widen — a process called vasodilation. When NO levels are healthy, your arteries stay flexible and blood pressure remains in a normal range. Research from Brigham and Women's Hospital and Harvard Medical School confirms that inhibition of NO synthesis in the vasculature can lead to hypertension.
Iron plays a dual role in this system. The enzyme that produces NO — endothelial nitric oxide synthase (eNOS) — requires a heme iron group to function. Without adequate iron, NO production can falter, potentially stiffening blood vessels. But excess iron creates the opposite problem: it generates reactive oxygen species that destroy NO before it can act, reducing its bioavailability and promoting vasoconstriction.
Iron Overload Versus Deficiency Effects
The cardiovascular system responds differently depending on whether iron is too low or too high. Iron deficiency forces compensatory mechanisms — faster heart rate, altered vascular resistance — that can shift blood pressure in either direction. Iron overload, on the other hand, promotes oxidative stress, damages vascular endothelium, and has been linked to cardiomyopathy and vascular dysfunction through excessive iron deposition in cardiac tissue.
Here are the key biological pathways through which blood pressure and iron interact:
- Hemoglobin-dependent oxygen delivery: Iron determines how much oxygen reaches tissues; reduced delivery triggers cardiovascular compensation that alters blood pressure.
- Nitric oxide metabolism: Iron is essential for NO synthesis via eNOS, but excess iron generates free radicals that neutralize NO and promote vessel stiffness.
- Reactive oxygen species (ROS) production: Surplus iron catalyzes Fenton reactions, producing hydroxyl radicals that damage endothelial cells and impair vascular relaxation.
- Sympathetic nervous system activation: When oxygen delivery drops due to low iron, the body increases sympathetic tone — raising heart rate and peripheral resistance.
- Cardiac iron deposition: In overload states, iron accumulates in heart muscle cells via L-type calcium channels, leading to diastolic dysfunction and arrhythmia susceptibility.
The takeaway: iron does not simply push blood pressure up or down. It modulates the machinery that controls vascular tone, oxygen delivery, and cardiac output. Whether that modulation helps or harms depends entirely on how much iron is circulating — and whether your body can handle it.
Iron Deficiency Anemia and Its Own Blood Pressure Effects
Here is a critical nuance most people miss: iron deficiency anemia itself changes your blood pressure — sometimes dramatically. So when you start taking iron tablets and notice your readings shift, the supplement may not be the direct cause. Instead, your body may be recalibrating as it corrects a deficiency that was already distorting your cardiovascular baseline.
Does anemia affect blood pressure? Absolutely. But the direction of that effect depends on severity, duration, and your body's compensatory capacity. Anemia can push blood pressure lower, higher, or create erratic swings between the two. Understanding this helps you separate what the iron tablet is doing from what the underlying deficiency was already doing.
When Anemia Causes Low Blood Pressure
Imagine your blood as a delivery fleet. With fewer functional red blood cells carrying oxygen, the fleet becomes less effective — even if the total blood volume stays roughly the same. Your tissues receive less oxygen per heartbeat, and the cardiovascular system struggles to maintain adequate perfusion pressure.
In mild to moderate iron deficiency anemia, the most common blood pressure response is a drop, particularly in systolic readings. The relationship between low iron and low blood pressure is well documented: reduced hemoglobin means reduced oxygen-carrying capacity, which translates to lower effective circulating volume from a functional standpoint. You might notice dizziness when standing, lightheadedness, or even fainting episodes — classic signs that does anemia causes low blood pressure in your case.
This hypotensive effect is especially pronounced during positional changes (orthostatic hypotension) because the body cannot compensate quickly enough when blood pools in the lower extremities. People with chronic mild anemia often adapt without realizing their "normal" blood pressure is actually suppressed by their iron status.
How Severe Anemia May Trigger Hypertension
This is where things get counterintuitive. Would anemia cause high blood pressure? In severe cases, yes — through a mechanism that seems paradoxical but makes physiological sense.
When hemoglobin drops significantly, your body activates emergency compensatory systems. A study published in Hypertension demonstrated that anemia significantly elevates sympathetic nerve activity — the fight-or-flight branch of your nervous system. Researchers found that patients with anemia had baseline muscle sympathetic nerve activity of 56.0 bursts per minute compared to 45.5 bursts per minute in matched controls without anemia. This heightened sympathetic drive increases heart rate, constricts peripheral blood vessels, and can push blood pressure upward.
The mechanism works through chemoreceptor activation. When tissues become hypoxic due to insufficient hemoglobin, peripheral chemoreceptors in the carotid bodies detect the oxygen deficit and trigger sympathetic outflow. The body essentially trades long-term vascular health for short-term oxygen delivery — raising pressure to force more blood through tissues that are starving for oxygen.
A 2024 study found a 2.5 times higher risk of iron-deficiency anemia in people with high blood pressure compared to those without, suggesting the relationship between anemia and high blood pressure runs in both directions. Can low iron cause hypertension? The evidence says it can — particularly when deficiency becomes severe enough to activate these compensatory pathways. The connection between anemia and hypertension is bidirectional, with each condition potentially worsening the other.
| Anemia Severity | Hemoglobin Range | Typical Blood Pressure Effect | Primary Mechanism |
|---|---|---|---|
| Mild (Hb 10-12 g/dL) | Slightly below normal | Mild decrease in systolic BP; possible orthostatic drops | Reduced oxygen-carrying capacity with minimal compensation |
| Moderate (Hb 8-10 g/dL) | Noticeably low | Variable — low BP at rest, possible spikes during exertion | Increased heart rate and cardiac output to maintain oxygen delivery |
| Severe (Hb below 8 g/dL) | Critically low | Elevated BP through sympathetic activation; risk of pulmonary hypertension | Chemoreflex-driven sympathetic overactivity, increased vascular resistance |
Blood Pressure Normalization After Correcting Deficiency
This is the piece that confuses most people taking iron supplements. When you begin correcting iron deficiency anemia, your blood pressure does not stay static — it shifts as your body dismantles the compensatory mechanisms it built during the deficiency period.
If your anemia was causing low blood pressure, starting iron tablets may bring your readings up toward a healthier baseline. You might interpret this as "iron raising my blood pressure," but what you are actually seeing is normalization — your cardiovascular system no longer needs to operate in a depleted state.
If your anemia was severe enough to trigger sympathetic-driven hypertension, correcting the deficiency should gradually reduce that compensatory overdrive. As hemoglobin rises and oxygen delivery improves, the chemoreceptor alarm quiets down, sympathetic tone decreases, and blood pressure may actually fall. Research confirms that anemia and blood pressure share this dynamic relationship — the readings you see during supplementation reflect a body in transition, not a static drug effect.
The timeline matters too. Blood pressure shifts during the first two to four weeks of supplementation are most likely related to this normalization process. Your body is rebuilding hemoglobin, restoring oxygen delivery, and recalibrating the autonomic nervous system. Can anemia cause high heart rate during this period? Yes — tachycardia is one of the last compensatory mechanisms to resolve, often persisting for several weeks after hemoglobin begins improving.
The practical implication: if your blood pressure changes after starting iron, the question is not just whether the supplement caused it. The more useful question is whether your body is correcting a pre-existing imbalance that was already distorting your cardiovascular function. Does hypertension cause anemia in some cases? Research suggests it can, creating a cycle where each condition feeds the other — making proper diagnosis and treatment of both conditions essential.

Different Iron Supplement Forms and Their Blood Pressure Impact
Not all iron supplements behave the same way inside your body. The form you take — whether it is a tablet, capsule, liquid, or intravenous infusion — determines how quickly iron enters your bloodstream, how much your body actually absorbs, and whether cardiovascular side effects are likely. If you have wondered whether can iron pills cause high blood pressure, the answer partly depends on which type of iron you are taking and how it is delivered.
Oral Iron Forms and Blood Pressure Profiles
Oral iron supplements come in several chemical forms, each with different elemental iron content and absorption characteristics. Ferrous sulfate contains about 20% elemental iron and remains the most widely prescribed option due to its low cost and proven efficacy. Ferrous fumarate delivers the highest elemental iron concentration at 33%, while ferrous gluconate sits lower at 12%. Iron bisglycinate chelate takes a different approach — bonding iron to two glycine molecules, which shields it from dietary inhibitors like phytates and tannins.
For most people taking standard oral doses, blood pressure effects are minimal. Oral iron enters the bloodstream gradually through intestinal absorption, avoiding the sudden systemic spikes that trigger cardiovascular responses. A randomized controlled trial comparing ferrous sulfate and iron bisglycinate chelate at 30 mg/day found no significant cardiovascular events with either compound over 90 days of supplementation. The primary differences between oral forms relate to gastrointestinal tolerability rather than blood pressure impact.
Does iron lower blood pressure when taken orally? In people with iron deficiency anemia who had compensatory hypertension, yes — correcting the deficiency can gradually reduce elevated readings as the body no longer needs sympathetic overdrive to maintain oxygen delivery. But this is normalization, not a pharmacological blood-pressure-lowering effect.
IV Iron Infusions and Acute Blood Pressure Changes
Intravenous iron is a different story entirely. When iron bypasses the gut and enters the bloodstream directly, the cardiovascular system faces a rapid change in circulating iron levels — and it responds accordingly.
A 2023 prospective cohort study of 950 hemodialysis patients found that iron sucrose administration during dialysis was independently associated with intradialytic hypertension. Patients receiving doses of 100 mg or more had a 7% higher rate of intradialytic hypertension (IRR 1.07, 95% CI 1.04-1.10) compared to those receiving no iron. Interestingly, the same study found an 11% lower rate of intradialytic hypotension in the higher-dose group (IRR 0.89, 95% CI 0.85-0.94), suggesting IV iron has vasoactive properties that shift blood pressure upward.
Can taking iron cause high blood pressure during an infusion? The evidence says yes — particularly with iron sucrose and ferric carboxymaltose. The mechanism likely involves iron's interaction with nitric oxide metabolism and its acute effects on vascular tone. Both hypertension and hypotension have been reported during IV iron administration, making close monitoring essential during infusions.
Which Format Carries the Lowest Cardiovascular Risk
For people concerned about blood pressure effects, oral iron forms — particularly chelated options like iron bisglycinate — carry the lowest cardiovascular risk. Their gradual absorption prevents the systemic iron spikes associated with IV administration. Research shows iron bisglycinate also produces fewer gastrointestinal side effects (21% vs. 37% for ferrous sulfate at equivalent doses), which improves long-term compliance without forcing patients toward higher-risk IV alternatives.
| Iron Form | Elemental Iron Content | Relative Bioavailability | Common Side Effects | Documented Blood Pressure Effects |
|---|---|---|---|---|
| Ferrous Sulfate (tablets) | 20% | Moderate | Nausea, constipation, stomach pain, dark stools | Minimal; no significant acute BP changes at standard doses |
| Ferrous Gluconate (tablets/capsules) | 12% | Moderate-Low | Milder GI effects than sulfate; metallic taste | Minimal; lower elemental iron reduces systemic load |
| Ferrous Fumarate (tablets) | 33% | Moderate-High | Higher GI side effects due to greater elemental iron | Minimal at standard doses; higher doses may increase cardiovascular stress |
| Iron Bisglycinate Chelate (capsules/tablets) | Variable (typically 20-26%) | High (resistant to dietary inhibitors) | Fewer GI complaints; better tolerated overall | Lowest oral cardiovascular impact; gentler systemic absorption |
| IV Iron Sucrose (infusion) | 100% (direct systemic delivery) | Complete (bypasses gut) | Infusion reactions, hypophosphatemia, headache | Associated with intradialytic hypertension (7% increased risk at doses ≥100 mg); may also reduce hypotension risk |
The format you choose matters beyond just blood pressure. Tablets and capsules offer controlled, gradual absorption that keeps systemic iron levels stable. For brands developing low blood pressure iron supplements or formulations targeting sensitive populations, the delivery format becomes a design decision with real clinical implications. Manufacturers offering multiple format options — such as ZhuFeng's OEM/ODM health food manufacturing services, which support production across hard capsules, tablets, soft capsules, oral liquids, and powder formats — allow supplement brands to select formulations optimized for gentler absorption profiles and reduced cardiovascular stress.
The bottom line: if you are worried about whether does iron lower blood pressure or raise it, the form and delivery method matter as much as the dose. Oral chelated iron offers the gentlest cardiovascular profile, standard ferrous salts remain safe for most people at therapeutic doses, and IV iron requires medical supervision specifically because of its documented acute blood pressure effects.

Who Faces Higher Risk of Blood Pressure Changes From Iron
The form and dosage of iron matter — but so does who is taking it. Your individual physiology determines how your cardiovascular system responds to supplementation. Some people can take standard iron doses without any measurable blood pressure shift. Others experience noticeable changes within the first few weeks. The difference often comes down to pre-existing conditions, life stage, and how much cardiovascular flexibility your body still has.
Five populations face disproportionate risk. If you belong to any of these groups, monitoring becomes essential rather than optional.
Pregnant Women and Cardiovascular Adaptation
Pregnancy already places enormous demands on the cardiovascular system. Blood volume increases by 30-50%, cardiac output rises, and vascular resistance drops to accommodate the growing placenta. Iron supplementation is routinely recommended during pregnancy to support fetal development and prevent anemia — but the cardiovascular context makes this population uniquely sensitive.
Research from Sinai Health's Lunenfeld-Tanenbaum Research Institute found that excess iron can harm the placenta, causing it to release harmful molecules into the bloodstream that damage blood vessels and impact blood pressure. The study, published in Circulation Research, demonstrated that iron overload in placental tissue triggers oxidative stress and cell death through ferroptosis — a process that releases toxic byproducts into maternal circulation and contributes to the hallmark hypertension of preeclampsia.
Preeclampsia affects up to 8% of all pregnancies and causes sudden blood pressure increases that threaten both mother and baby. The researchers noted that managing iron levels could represent a new approach to preventing this condition.
- Why pregnant women are more susceptible: Already-expanded blood volume and altered vascular tone create a cardiovascular system operating near its adaptive limits; excess iron adds oxidative stress to an already-strained placenta.
- Key risk factor: Iron overload combined with insufficient antioxidant defenses precipitates harmful molecule production that impairs placental function and damages maternal blood vessels.
- Precautions: Do not self-prescribe iron doses above what your prenatal provider recommends. Request ferritin testing before increasing supplementation. Report any sudden blood pressure changes, headaches, or visual disturbances immediately — these may signal preeclampsia rather than a benign supplement effect.
Elderly Patients and Vascular Sensitivity
Aging changes the rules. Blood vessels lose elasticity, arterial walls stiffen, and the baroreceptor reflex — your body's built-in blood pressure stabilizer — becomes less responsive. When an elderly person takes iron supplements, their cardiovascular system has less capacity to buffer any changes in vascular tone or blood volume dynamics.
Older adults are also more likely to have iron-poor diets and indolent gastrointestinal blood loss from gastritis or underlying malignancy, making iron supplementation common in this group. Yet the combination of reduced vascular flexibility and higher baseline cardiovascular risk means even modest iron-related changes can produce clinically meaningful blood pressure shifts.
The relationship between anemia and hypertension is particularly relevant here. Many elderly patients present with both conditions simultaneously — iron deficiency driving compensatory cardiovascular strain while age-related arterial stiffness independently elevates blood pressure. Correcting the anemia may improve one mechanism while the underlying vascular rigidity persists.
- Why elderly individuals are more susceptible: Reduced arterial compliance means blood vessels cannot easily accommodate changes in blood flow dynamics; diminished baroreceptor sensitivity slows the body's ability to correct pressure fluctuations.
- Key risk factor: Polypharmacy — elderly patients often take multiple medications including antihypertensives, and iron can interact with drug absorption and metabolism.
- Precautions: Start with lower iron doses and titrate gradually. Monitor blood pressure weekly during the first month of supplementation. Take iron at least two hours apart from blood pressure medications to avoid absorption interference. Report dizziness, headaches, or unusual fatigue to your provider.
Pre-Existing Hypertension and Iron Supplementation
This is the group with the strongest research evidence for concern. A UK Biobank study of 427,939 participants found that habitual iron supplementation was associated with a significantly higher risk of chronic kidney disease in hypertensive individuals (HR 1.12, 95% CI 1.02-1.22) — and the risk jumped further in those taking antihypertensive medication (HR 1.21, 95% CI 1.08-1.35). In normotensive participants, no significant association existed.
The mechanism likely involves iron-induced oxidative stress compounding the vascular damage already present in hypertension. Excess iron catalyzes Fenton reactions that produce reactive oxygen species, which destroy nitric oxide and promote vasoconstriction. In someone whose blood vessels are already under strain from elevated pressure, this additional oxidative burden can accelerate vascular injury. Does hypertension cause anemia in some patients? It can — particularly through kidney damage that impairs erythropoietin production — creating a cycle where treating one condition with iron supplementation may inadvertently stress the other.
The study also revealed significant interactions between iron supplementation and antihypertensive medication use. The combined effect exceeded what either factor would produce alone, suggesting iron may alter how blood pressure medications work — possibly through iron-drug chelation or by counteracting the antioxidant properties of certain antihypertensives.
- Why hypertensive individuals are more susceptible: Already-elevated oxidative stress and vascular inflammation create a system where additional iron-driven free radical production compounds existing damage; iron deficiency hypertension may mask the true baseline, complicating monitoring.
- Key risk factor: Concurrent use of antihypertensive medication — the UK Biobank data showed a 21% increased CKD risk in this specific subgroup, with significant multiplicative and additive interactions between iron and blood pressure drugs.
- Precautions: Discuss iron supplementation explicitly with your prescribing physician. Request baseline kidney function tests before starting. Monitor blood pressure more frequently — at least twice weekly during the first month. Consider lower doses or chelated iron forms that produce less oxidative stress. Never adjust blood pressure medication doses based on readings taken during the initial weeks of iron supplementation without medical guidance.
Two additional groups deserve attention. People with chronic kidney disease face altered iron metabolism — their kidneys cannot produce adequate erythropoietin, and iron handling becomes dysregulated. IV iron is commonly used in this population, but as discussed in the previous section, it carries documented acute blood pressure effects. Athletes using high-dose iron supplementation to boost performance also face elevated risk, as supraphysiological doses can overwhelm the body's iron-buffering systems and generate oxidative stress that affects vascular function during intense exercise.
The common thread across all these populations: a cardiovascular system already operating under stress — whether from pregnancy, aging, disease, medication, or extreme physical demand — has less margin to absorb the metabolic effects of iron supplementation. The question of whether can anemia cause hypertension becomes especially relevant in these groups, because the interplay between deficiency, supplementation, and pre-existing cardiovascular strain creates a more complex clinical picture than in healthy adults.
Knowing your risk category is the first step. The next consideration is how much iron you are actually taking — because dosage thresholds determine whether these theoretical risks translate into measurable blood pressure changes.
Dosage Thresholds and Whether Blood Pressure Effects Are Temporary
Risk category matters, but so does the amount of iron entering your system each day. A person with pre-existing hypertension taking 18 mg of elemental iron in a multivitamin faces a very different cardiovascular equation than someone prescribed 200 mg daily for severe anemia. The dose determines whether iron remains a quiet nutrient or becomes a metabolic stressor capable of shifting your blood pressure readings.
Standard Versus High-Dose Iron and Cardiovascular Response
Standard therapeutic doses for iron deficiency anemia typically range from 65 to 200 mg of elemental iron per day. A common prescription is one 325 mg ferrous sulfate tablet taken one to three times daily — delivering roughly 65 to 195 mg of elemental iron. At these levels, most people experience gastrointestinal side effects long before any cardiovascular changes appear. According to StatPearls clinical guidance, amounts up to 20 mg/kg of elemental iron are generally well tolerated, with only mild GI symptoms. Between 20 and 60 mg/kg, toxicity becomes mild to moderate, and above 60 mg/kg, severe symptoms including tachycardia, metabolic acidosis, and circulatory collapse can occur.
For context, a 70 kg adult would need to ingest over 1,400 mg of elemental iron in a single sitting to reach the 20 mg/kg threshold — far beyond any prescribed daily dose. So at standard therapeutic levels, the direct cardiovascular risk from a single dose is negligible. The concern with iron deficiency and hypertension is not acute toxicity but rather cumulative effects over weeks or months of supplementation, particularly in vulnerable populations.
High-dose protocols — sometimes used for rapid repletion or in athletes seeking performance gains — compress more iron into a shorter timeframe. This increases the likelihood that systemic iron levels temporarily exceed what the body can safely process, generating oxidative stress that may affect vascular tone. The relationship between high iron and high blood pressure becomes more relevant at these elevated doses, where the body's iron-buffering capacity (ferritin storage, transferrin binding) approaches saturation.
Timeline of Blood Pressure Changes During Supplementation
When blood pressure shifts do occur during iron supplementation, they follow a fairly predictable pattern:
- Days 1-7: Minimal systemic change. Iron is being absorbed and incorporated into ferritin stores. Blood pressure readings typically remain stable.
- Weeks 2-4: Hemoglobin begins rising. If anemia was present, compensatory mechanisms start unwinding — heart rate may decrease, vascular resistance shifts, and blood pressure readings begin moving toward a new baseline. This is the window where most people notice changes.
- Weeks 4-8: Blood counts return to normal for most people after two months of therapy. Cardiovascular compensation largely resolves. Blood pressure stabilizes at what should be a healthier equilibrium.
- Months 3-12: Continued supplementation rebuilds bone marrow iron stores. If blood pressure remains elevated beyond the initial normalization period, the cause is unlikely to be iron alone — other factors warrant investigation.
The pattern of high iron low blood pressure can also emerge during this timeline. As severe anemia resolves and sympathetic overdrive quiets, someone whose body was compensating with elevated pressure may see readings drop — sometimes below their expected baseline — before stabilizing. This transient dip reflects the lag between hemoglobin recovery and full autonomic recalibration.
When Effects Resolve After Stopping or Adjusting Dose
The reassuring reality: most blood pressure changes linked to iron supplementation are temporary. They resolve either when the body finishes adjusting to improved iron status or when supplementation ends. Iron does not accumulate indefinitely in healthy people — the body downregulates intestinal absorption through hepcidin signaling once stores are replete.
However, one scenario produces persistent cardiovascular effects: iron overload. Hemochromatosis — whether hereditary or secondary to excessive supplementation — causes iron to deposit in organs including the heart. Cleveland Clinic notes that iron overload especially damages the heart, liver, and pancreas, and can lead to congestive heart failure and arrhythmias. The connection between high iron and high blood pressure becomes clinically significant in overload states, where iron-driven oxidative damage to blood vessel walls promotes chronic vascular stiffness and sustained hypertension.
Hereditary hemochromatosis affects roughly 1 in 200 people of Northern European descent. If you are supplementing iron without confirmed deficiency, or if your ferritin levels climb above the normal range during treatment, the risk of inadvertently pushing toward overload — and its cardiovascular consequences — increases. Symptoms often do not appear until your 40s or 50s, meaning damage can accumulate silently for years.
The practical rule: if your blood pressure normalizes within 6-8 weeks of starting iron, the shift was almost certainly part of your body's recalibration. If readings remain elevated beyond that window — or if they climb progressively — request ferritin and transferrin saturation testing to rule out overload. Persistent high iron low blood pressure after stopping supplementation also warrants evaluation, as it may indicate autonomic dysfunction unrelated to iron status.

How to Monitor Blood Pressure While Taking Iron Supplements
Knowing that blood pressure shifts can happen during iron supplementation is useful. Knowing exactly what to do about it is better. Whether you fall into a higher-risk category or simply want peace of mind, a structured monitoring approach removes the guesswork and helps you catch meaningful changes before they become problems.
You do not need expensive equipment or medical training. A validated home blood pressure monitor, a simple log, and a clear protocol are enough to track what matters. The American Heart Association recommends sitting in a chair with back support, both feet flat on the ground, arm extended and supported at heart level, staying quiet and still for accurate readings.
A Practical Blood Pressure Monitoring Schedule
Timing matters. Random spot-checks tell you very little — what you need is a consistent pattern that reveals trends over time. Here is a step-by-step protocol designed specifically for people starting iron supplementation:
- Establish a baseline before starting iron. Take readings at the same time each morning and evening for three consecutive days before your first dose. Record all six readings. Average them separately for morning and evening — these numbers become your reference point.
- Monitor weekly during the first month. Take two readings (morning and evening) on the same day each week. Compare against your baseline. This is the window where most cardiovascular adjustments occur as hemoglobin begins rising and compensatory mechanisms unwind.
- Shift to biweekly checks during weeks 5-8. If your readings have remained stable through the first month, reduce frequency but maintain consistency. The body is still recalibrating iron stores during this period.
- Move to monthly monitoring after week 8. By this point, blood counts have typically normalized and cardiovascular compensation has resolved. Monthly checks confirm stability and catch any late-emerging patterns.
- Resume weekly monitoring if you change dose or iron form. Any adjustment to your supplementation protocol resets the clock — your body needs time to adapt to the new input.
Can low iron affect blood pressure readings independently of supplementation? Yes — and this is exactly why the baseline measurement matters so much. If your pre-supplement readings were already distorted by anemia, the changes you see after starting iron reflect normalization rather than a new problem. Without that baseline, you have no way to distinguish the two.
Warning Signs That Require Medical Attention
Not every blood pressure fluctuation during iron supplementation is cause for alarm. A reading that is 3-5 mmHg higher than your baseline on a single day could reflect caffeine, stress, poor sleep, or measurement technique. What matters is the pattern — sustained, directional changes that persist across multiple readings.
Seek medical attention if your systolic blood pressure rises more than 10 mmHg above baseline and stays elevated across three or more consecutive measurement sessions, if you experience readings above 180/120 mmHg at any point, or if blood pressure changes are accompanied by chest pain, severe headache, visual disturbances, shortness of breath, or significant swelling.
Can anemia affect blood pressure in ways that mimic dangerous symptoms? It can. Dizziness, rapid heartbeat, and lightheadedness overlap between anemia-related blood pressure changes and more serious cardiovascular events. The distinguishing factor is persistence and severity. Transient lightheadedness when standing that resolves within seconds is typical of anemia correction. Sustained dizziness with visual changes or chest pressure is not.
Can anemia cause high heart rate even after starting iron? Yes — tachycardia is often one of the last compensatory mechanisms to resolve. Your heart rate may remain elevated for several weeks after hemoglobin begins improving because the autonomic nervous system recalibrates more slowly than red blood cell production. A resting heart rate that stays above 100 bpm for more than four weeks after starting supplementation, or one that increases rather than decreases over time, warrants a conversation with your provider.
The 2025 AHA/ACC hypertension guideline sets a treatment target of less than 130/80 mmHg for all patients. If your readings consistently exceed this threshold during supplementation — particularly if they were below it at baseline — that is a signal worth discussing with your doctor regardless of whether iron is the suspected cause.
How to Discuss Iron and Blood Pressure With Your Doctor
Bringing data to your appointment changes the conversation. Instead of saying "I think my iron pills are raising my blood pressure," you can show a log with dated readings, your pre-supplement baseline, and the exact timeline of changes. This gives your provider the information needed to make a clinical judgment rather than a guess.
Here is what to prepare:
- Your baseline readings (pre-supplementation averages for morning and evening)
- Weekly readings since starting iron, with dates and times noted
- The specific iron form, dose, and brand you are taking
- Any other supplements or medications started around the same time
- Symptoms you have noticed — including timing relative to iron doses
Can anemia make you faint during the adjustment period? It is possible, particularly if you had orthostatic hypotension from anemia that is now resolving unevenly. Mention any episodes of near-fainting or actual syncope — these help your doctor determine whether your autonomic nervous system is recalibrating normally or whether something else is happening.
Your provider may order ferritin and transferrin saturation tests to confirm your iron stores are rising appropriately without tipping toward overload. They may also adjust your dose, switch your iron form, or space doses differently based on your blood pressure pattern. The goal is not to stop iron supplementation unnecessarily — it is to find the approach that corrects your deficiency without creating a new cardiovascular concern.
Monitoring gives you control over a process that otherwise feels invisible. But the quality of the supplement itself also plays a role in how your body responds — because not all iron formulations are created with the same attention to absorption kinetics and tolerability.
Why Supplement Formulation and Quality Affect Your Response
Two iron supplements can list the same elemental iron content on their labels and produce completely different experiences inside your body. One might absorb smoothly with minimal side effects. The other might flood your system with unbound iron, trigger GI distress, and create the kind of systemic oxidative stress that nudges blood pressure readings upward. The difference comes down to formulation — how the iron is prepared, what it is paired with, and how the delivery mechanism controls its release.
When you are concerned about iron and high blood pressure, the quality of your supplement is not a marketing detail. It is a physiological variable that determines how much cardiovascular stress each dose creates.
Formulation Factors That Reduce Side Effects
Think of iron absorption like water flowing through a pipe. A well-designed supplement delivers iron at a rate your intestinal cells can handle — steady, controlled, manageable. A poorly formulated one opens the floodgates, overwhelming absorptive capacity and leaving excess unbound iron to irritate the gut lining and generate free radicals systemically.
Several formulation decisions directly influence how gently iron enters your bloodstream and how much oxidative burden it places on your cardiovascular system:
- Iron form and chelation: Chelated forms like iron bisglycinate wrap the iron atom in amino acid bonds that protect it from interacting with food inhibitors and reduce direct contact with the intestinal mucosa. This means less GI irritation and more predictable absorption — avoiding the erratic spikes in serum iron that can stress blood vessels. Non-chelated ferrous salts dissolve freely in stomach acid, which improves availability but also increases the chance of unabsorbed iron generating reactive oxygen species in the gut.
- Controlled-release technology: Some formulations use enteric coatings or matrix-based slow-release systems that distribute iron absorption over several hours rather than delivering the full dose in one burst. This reduces peak serum iron levels and gives the body's transferrin-binding system time to sequester incoming iron safely — lowering the oxidative load on vascular endothelium.
- Complementary nutrients for absorption: Vitamin C (ascorbic acid) reduces ferric iron (Fe3+) to the more absorbable ferrous form (Fe2+) and helps prevent the formation of insoluble iron compounds in the gut. Clinical evidence on vitamin C as an absorption enhancer is mixed but mechanistically sound — it prevents insoluble iron compound formation and maintains iron in its reduced state. Including it in the formulation rather than relying on dietary intake ensures consistent enhancement.
- Avoidance of absorption inhibitors: Calcium, tannins from tea and coffee, and high-fiber binders all reduce iron uptake. A well-designed supplement accounts for these interactions — either through chelation that shields iron from inhibitors or through clear dosing instructions that separate iron from interfering substances. The evidence against tea and coffee is clear and consistent: both are potent inhibitors and should be avoided within one hour of taking oral iron.
- Appropriate elemental iron content: More is not better. Research on hepcidin dynamics shows that oral iron ingestion raises hepcidin levels for up to 48 hours, suppressing further absorption during that window. Formulations delivering excessive elemental iron per dose simply increase the unabsorbed fraction — which causes GI side effects without improving iron status. Every-other-day dosing at moderate amounts often outperforms daily high-dose regimens in both tolerability and net absorption.
- Binding agents and excipients: Inferior fillers, binders, or coating materials can alter dissolution rates unpredictably. Some low-quality tablets disintegrate too quickly (dumping iron), while others pass through the GI tract partially intact (wasting iron). Either scenario disrupts the controlled absorption profile that minimizes cardiovascular stress.
The relationship between low iron and blood pressure is complex enough without adding formulation variables that make your body's response less predictable. Each of these factors either smooths or disrupts the absorption curve — and smoother absorption means less systemic stress per dose.
What to Look for in a Well-Designed Iron Supplement
If you are choosing iron for blood pressure safety alongside deficiency correction, a few practical markers separate thoughtful formulations from generic ones:
Look for supplements that specify the iron form (not just "iron" on the label), include vitamin C or another absorption enhancer, state the elemental iron content clearly, and use dosing schedules aligned with current evidence — once daily or every other day rather than multiple times per day. A 2026 clinical review confirmed that no single oral iron formulation demonstrates clear superiority in efficacy, but tolerability differences are real and clinically meaningful. Gastrointestinal side effects affect up to 10% of patients and significantly impact adherence — making formulation quality a practical determinant of treatment success.
For brands developing iron supplements aimed at sensitive populations — pregnant women, elderly patients, or those managing iron and high blood pressure simultaneously — the manufacturing process itself becomes critical. Customized formulation requires expertise in selecting the right iron form, pairing it with synergistic nutrients, and delivering it in a format that matches the target population's needs. Experienced OEM manufacturers who offer flexible production across multiple formats enable this kind of precision. ZhuFeng's OEM/ODM health food manufacturing services, for example, support scalable production across tablets, hard capsules, soft capsules, oral liquids, and powder formats — allowing brands to develop gentler, better-absorbed iron products tailored to populations where cardiovascular safety is a priority.
The bottom line: whether can iron tablets increase blood pressure in your specific case depends not just on dose and duration, but on how intelligently the supplement was designed. A well-formulated product delivers iron at a pace your body can handle, pairs it with nutrients that optimize uptake, and avoids the absorption spikes that generate unnecessary oxidative stress. That is the difference between a supplement that quietly corrects your deficiency and one that creates new concerns along the way.
Frequently Asked Questions About Iron Tablets and Blood Pressure
1. Can iron supplements cause high blood pressure in healthy people?
For most healthy individuals, iron supplements at standard therapeutic doses (65-200 mg elemental iron daily) do not cause high blood pressure. Research from the UK Biobank study of over 427,000 participants found no significant adverse cardiovascular association in normotensive individuals. Blood pressure changes are more likely in people with pre-existing hypertension, those taking antihypertensive medications, or individuals prone to iron overload. If you are healthy with confirmed iron deficiency, standard oral supplementation carries minimal cardiovascular risk when taken as directed.
2. Does iron deficiency anemia cause low or high blood pressure?
Iron deficiency anemia can cause both low and high blood pressure depending on severity. Mild to moderate anemia typically lowers blood pressure due to reduced oxygen-carrying capacity, causing symptoms like dizziness and lightheadedness. Severe anemia (hemoglobin below 8 g/dL) can paradoxically trigger hypertension through sympathetic nervous system activation, as the body increases vascular resistance to force more oxygen to starving tissues. When you start iron tablets, blood pressure may shift as your body dismantles these compensatory mechanisms rather than from a direct supplement effect.
3. Which iron supplement form is safest for people concerned about blood pressure?
Iron bisglycinate chelate carries the lowest cardiovascular risk among oral iron forms. Its chelated structure allows gradual, predictable absorption without the serum iron spikes that generate oxidative stress on blood vessels. Clinical trials show it produces fewer gastrointestinal side effects (21% vs. 37% for ferrous sulfate) while maintaining good bioavailability. IV iron carries the highest blood pressure risk, with studies showing a 7% increased rate of hypertension during infusions at doses of 100 mg or more. For brands developing iron products for sensitive populations, working with experienced OEM manufacturers like ZhuFeng (https://en.ahzfsw.com/service.html) enables customized formulations across multiple formats optimized for gentler absorption.
4. How long do blood pressure changes last after starting iron supplements?
Most blood pressure changes during iron supplementation are temporary and follow a predictable timeline. Shifts typically appear during weeks 2-4 as hemoglobin rises and cardiovascular compensation unwinds. Blood counts generally normalize by week 8, and blood pressure stabilizes at a healthier baseline. If readings remain elevated beyond 6-8 weeks, the cause is unlikely to be iron alone and warrants ferritin testing to rule out iron overload. Persistent changes may indicate hemochromatosis or other underlying conditions requiring medical evaluation.
5. Should I monitor my blood pressure when taking iron tablets?
Yes, especially if you belong to a higher-risk group (pregnant women, elderly individuals, those with pre-existing hypertension, or chronic kidney disease patients). Establish a baseline by taking morning and evening readings for three days before starting iron. Monitor weekly during the first month, biweekly during weeks 5-8, then monthly thereafter. Seek medical attention if systolic blood pressure rises more than 10 mmHg above baseline across three or more consecutive sessions, or if changes are accompanied by chest pain, severe headache, visual disturbances, or shortness of breath.