

What Extended Release Tablets Actually Are
You pick up your prescription, glance at the label, and notice the letters "ER" or "XR" after the drug name. What does extended release mean, exactly? And how do extended release tablets work differently from a standard pill?
What Does Extended Release Mean
Extended release means a tablet is formulated so the active ingredient is released gradually over many hours, maintaining steady drug levels in the bloodstream instead of delivering the entire dose at once.
That's the simplest definition of extended release you'll find, and it captures the core idea. A standard immediate-release pill dumps its full payload into your system within minutes. An extended release tablet, by contrast, uses physical or chemical barriers to meter out medication slowly, often over 12 to 24 hours. The result is fewer daily doses and a smoother ride for your body.
To define extended release in practical terms: imagine the difference between gulping an entire glass of water at once versus sipping it steadily throughout the day. Your body handles the steady approach much more gracefully.
Why ER Tablets Are So Common Today
Extended release formulations are far from niche. Roughly one-third of all oral medications prescribed today use some form of controlled-release technology. You'll find them across nearly every therapeutic category, from cardiovascular drugs and diabetes medications to psychiatric treatments and pain management.
Why so popular? The extended release meaning goes beyond convenience. These formulations exist because keeping drug levels consistent in the bloodstream directly translates to better outcomes: fewer side effects from concentration spikes, less risk of the drug dropping below effective levels between doses, and improved patient adherence since taking one pill a day is easier than remembering three or four.
All of these benefits hinge on a single pharmacological concept that governs how every medication works in your body: the therapeutic window. Staying inside that window is the entire reason extended release technology exists, and understanding it changes how you think about every pill you take.
The Therapeutic Window and Why Steady Blood Levels Matter
Every medication has a sweet spot in your bloodstream. Too little and it does nothing. Too much and you risk harmful side effects. The range between those two boundaries is what pharmacologists call the therapeutic window, and it's the single most important concept for understanding why extended release vs immediate release formulations behave so differently inside your body.
Understanding the Therapeutic Window
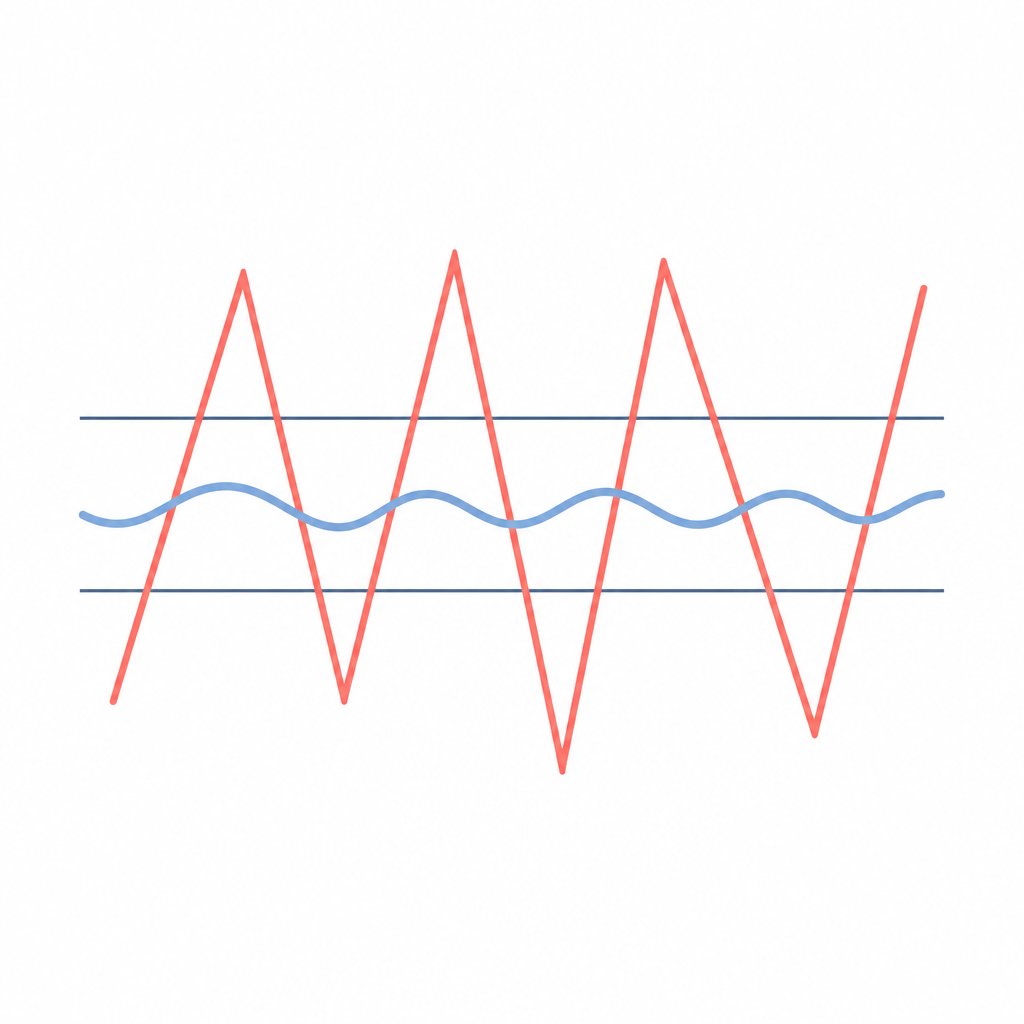
Picture two invisible lines on a graph tracking drug concentration in your blood over time. The lower line is the minimum effective concentration (MEC), the threshold below which the drug simply isn't doing its job. The upper line is the maximum tolerated concentration (MTC), the ceiling above which side effects become likely or dangerous. Your medication needs to stay between those two lines to work safely.
Here's what happens at each level:
- Above the therapeutic window: Drug concentration exceeds the MTC. You're at increased risk of toxicity, adverse reactions, and dose-related side effects like nausea, dizziness, or organ stress.
- Within the therapeutic window: The drug is both effective and safe. Symptoms are managed, and side effects remain minimal. This is the target zone.
- Below the therapeutic window: Concentration drops under the MEC. The medication loses its therapeutic effect, symptoms return, and the condition goes untreated until the next dose kicks in.
The narrower a drug's therapeutic window, the more critical it becomes to keep blood levels steady. This is exactly why therapeutic drug monitoring exists for certain medications: even small fluctuations can push a patient above or below the safe zone.
Peaks and Troughs Explained Simply
When you take an immediate release tablet, the drug floods into your bloodstream quickly. What is immediate release in practical terms? It means the full dose dissolves and absorbs within minutes, producing a sharp spike in plasma concentration. That spike often overshoots the therapeutic window before the body metabolizes the drug and levels crash back down, sometimes dipping below the effective threshold well before your next scheduled dose.
This pattern of rapid peaks and deep troughs repeats with every dose. A pharmacokinetic study comparing IR and ER formulations of carbidopa-levodopa illustrates this clearly: the immediate release version reached peak plasma concentration within one hour, then dropped to less than 10% of that peak by five hours. The extended release formulation, by contrast, sustained concentrations above 50% of its peak for nearly five hours and didn't fall to 10% of peak until past ten hours (Hsu et al., J Clin Pharmacol, 2015).
Think of it this way. Immediate release is like turning a faucet on full blast, filling the sink past the overflow line, then shutting it off completely and waiting until the basin is nearly empty before blasting it again. Extended release is like a slow, steady drip that keeps the water level right where you want it, never flooding, never running dry.
When you compare instant release vs extended release on a plasma concentration curve, the difference is striking. The IR curve looks like a series of sharp mountain peaks and valleys. The ER curve looks more like a gently rolling plateau. That flatter profile means the drug spends far more time inside the therapeutic window and far less time in the danger zones above or below it.
This matters beyond comfort. Research on conditions like Parkinson's disease shows that continuous, steady drug delivery reduces motor complications compared to the pulsatile pattern of instant release vs extended-release dosing. The variability in plasma concentration with IR formulations can be more than double that of ER versions, measured by the coefficient of variation in blood levels over time.
In the IR vs ER comparison, the tradeoff is straightforward: immediate release gives you a faster onset but a rougher ride, while extended release sacrifices a few minutes of speed for hours of stability. For chronic conditions requiring round-the-clock management, that stability is exactly what keeps patients feeling well between doses.
Steady blood levels are the goal. But how does a single tablet actually achieve that slow, controlled release as it travels through your digestive system? The answer lies in what physically happens to the tablet after you swallow it.
What Happens Inside Your Body After You Swallow an ER Tablet
You swallow an extended release tablet with a glass of water. Within seconds it's past your throat and on its way. But how do tablets work once they're inside you? The journey from mouth to full absorption is a carefully orchestrated process that can span anywhere from 12 to 24 hours, depending on the formulation.
From Swallowing to Absorption Step by Step
If you've ever wondered how long does it take for a pill to dissolve or how long does it take for pills to absorb, the answer for ER tablets is deliberately slow. Unlike immediate release pills that break apart within minutes, an extended release tablet is engineered to resist rapid dissolution and release its contents gradually as it travels through your entire gastrointestinal tract.
Here's what happens at each stage of the journey:
- Mouth and esophagus (seconds): The tablet passes through quickly. No meaningful dissolution occurs here. This is why you're told to swallow ER tablets whole with plenty of water, ensuring the tablet reaches the stomach intact.
- Stomach (30 minutes to 2 hours): Gastric acid and fluids begin working on the tablet's outer protective coating. Many ER tablets have an enteric or pH-sensitive film that resists the acidic stomach environment, preventing premature drug release. For matrix-type tablets, the outer polymer layer starts to hydrate.
- Upper small intestine (2 to 6 hours): As the tablet moves into the duodenum and jejunum, the pH rises and conditions shift. The matrix swells as it absorbs intestinal fluid, forming a gel-like barrier. Drug molecules begin diffusing outward through this gel layer at a controlled rate. Absorption into the bloodstream starts here in earnest.
- Lower small intestine and ileum (4 to 10 hours): The tablet continues eroding or releasing drug through diffusion and osmotic mechanisms. Pharmaco-scintigraphic studies show that some extended release formulations don't begin significant disintegration until they reach the ileum, roughly 5 to 10 hours after swallowing.
- Colon (8 to 24 hours): Whatever remains of the tablet continues releasing drug as it passes through the ascending and transverse colon. By this point, most of the active ingredient has been absorbed. The depleted tablet structure, now largely inert, moves toward elimination.
How long do pills take to digest in this extended release format? The entire transit from swallowing to elimination typically takes 12 to 24 hours, though individual variation in gut motility, food intake, and tablet design all influence timing. The key difference from standard pills is that absorption isn't a single event. It's a continuous process spread across the full length of your digestive system.
Why You Might See a Tablet Shell in Your Stool
Here's something that catches many patients off guard: you might notice what looks like a whole tablet in your stool after taking certain ER medications. This is completely normal and has a name: the ghost pill phenomenon.
Certain ER tablets, particularly those using osmotic pump technology, are housed in a rigid, insoluble shell. The shell has a tiny laser-drilled hole through which the drug is pushed out by osmotic pressure as the tablet travels through your gut. Once all the medication has been expelled, the empty shell passes through intact. It looks like an undissolved pill, but the active drug has already been fully absorbed into your bloodstream.
Medications like methylphenidate (Concerta), paliperidone (Invega), and some venlafaxine extended release tablets are well-documented examples. Their prescribing information explicitly states that patients may see empty shells in their stool and that this is expected. A clinical review in Therapeutic Advances in Drug Safety found that lack of awareness about ghost pills caused significant anxiety in patients who believed their medication wasn't being absorbed.
If you notice this, don't panic and don't stop taking your medication. The shell you're seeing is just the delivery vehicle after it has done its job. If you have concerns about how long does it take pills to digest or whether your specific medication is absorbing properly, your pharmacist can confirm whether your ER formulation is one that produces ghost pills.
The ghost shell is a visible clue to something invisible: the sophisticated engineering inside each tablet that controls exactly how and when drug molecules escape. That engineering comes in several distinct forms, each using a different physical principle to achieve the same goal of slow, steady release.

Four Types of Extended Release Mechanisms Explained
Not all extended release tablets use the same trick to slow down drug delivery. Pharmaceutical engineers have developed several distinct approaches to achieve that steady, controlled release, each relying on a different physical principle. Understanding how do slow release tablets work at a mechanical level helps explain why these formulations come with such strict handling instructions.
Matrix Tablets and the Sponge Analogy
The most common type of time release tablets uses a matrix system. Imagine a kitchen sponge soaked with water. When you squeeze it gently, water seeps out slowly and evenly rather than gushing all at once. A matrix tablet works on the same principle.
The drug is embedded throughout a grid of polymer excipients. When the tablet reaches your digestive tract and absorbs fluid, this polymer network swells and forms a gel layer around the tablet core. The medication then diffuses outward through that gel barrier at a controlled, predictable rate. Colorcon's formulation research identifies three main subtypes: hydrophilic matrices that swell with water-soluble polymers, lipophilic matrices that erode slowly using water-insoluble materials, and bi-layer matrices that combine an immediate-release layer with an extended-release layer for dual release kinetics.
Matrix systems are popular because they're relatively simple to manufacture and can accommodate high drug loads. They represent the most widely used technology in extended drug release, found in everything from cardiovascular medications to sustained release capsules for pain management.
Osmotic Pump Systems and Coated Bead Capsules
Osmotic pump tablets, often called OROS (Oral Osmotic System), are the most precisely engineered of all extended release tablets. Think of them as tiny pressure-driven engines.
Here's how they work: the tablet core is surrounded by a rigid, semi-permeable membrane. A laser-drilled orifice (typically 0.075 to 0.274 mm in diameter) is created in that membrane. When the tablet enters your GI tract, water is drawn through the membrane by osmotic pressure, dissolving the drug inside. As internal pressure builds, the drug solution is pushed out through the tiny hole at a constant, predictable rate, independent of pH or gut motility. This is the mechanism that produces those ghost shells discussed earlier.
Coated bead capsules take a completely different approach. Instead of one monolithic tablet, these extended release capsules contain hundreds of tiny pellets or beads, each coated with polymer layers of varying thickness. Thin-coated beads dissolve quickly, medium-coated beads release drug a few hours later, and thick-coated beads hold their payload until much later in the GI transit. The staggered dissolution creates a smooth, sustained release profile from what looks like a simple capsule. Many time release capsules for ADHD medications and antidepressants use this multi-particulate design.
The fourth mechanism, hydrophilic gel systems, relies on polymers like hydroxypropyl methylcellulose (HPMC). When these polymers contact intestinal fluid, they form a viscous gel barrier that controls how fast drug molecules can diffuse outward. Research published in the Saudi Pharmaceutical Journal demonstrates that HPMC-based matrices can extend drug release beyond 8 hours, with higher viscosity grades producing thicker gel layers and slower release rates. The gel essentially acts as a rate-limiting gatekeeper between the drug core and your bloodstream.
| Mechanism | How It Works | Common Medication Category |
|---|---|---|
| Matrix System | Drug embedded in a polymer grid that swells and releases medication through gradual diffusion and erosion | Cardiovascular drugs, diabetes medications |
| Osmotic Pump (OROS) | Semi-permeable membrane with a laser-drilled hole; osmotic pressure pushes drug out at a constant rate | ADHD medications, antipsychotics |
| Coated Bead/Pellet Capsules | Hundreds of tiny beads with different coating thicknesses dissolve at staggered intervals | Antidepressants, ADHD medications |
| Hydrophilic Gel (HPMC) | Polymer forms a viscous gel barrier on contact with fluid, controlling drug diffusion rate | Pain management, antihypertensives |
Each of these mechanisms achieves the same fundamental goal: keeping drug release slow and steady so your blood levels stay within the therapeutic window. But they differ in precision, manufacturing complexity, and how they respond to the variable conditions inside your digestive tract. These differences also explain why the same drug might carry different abbreviations on the label depending on which release technology it uses.
ER vs SR vs CR vs DR and What the Letters on Your Bottle Mean
You've seen how different mechanisms control drug release inside a tablet. But when you look at your prescription bottle, you're not seeing mechanism names. You're seeing abbreviations like ER, XR, SR, CR, or DR, and it's easy to assume each one represents a fundamentally different technology. The reality is simpler than the alphabet soup suggests.
IR vs ER vs SR vs CR at a Glance
When comparing sustained release vs extended release, or controlled release vs extended release, the honest answer is that these terms overlap significantly. ER, XR, XL, SR, and CR all describe formulations designed to release medication slowly over an extended period. The differences between them are often more about branding and regulatory naming conventions than about distinct mechanisms inside the tablet.
Here's how the main categories break down:
- Immediate Release (IR): The drug dissolves and absorbs rapidly. You get fast onset but short duration, typically requiring multiple daily doses.
- Extended Release (ER/XR/XL): An umbrella term for any formulation that prolongs drug release, usually maintaining therapeutic levels for 8 to 12 hours or longer compared to 4 to 6 hours for IR versions.
- Sustained Release (SR): Releases medication over a sustained period but not necessarily at a precisely controlled rate. Functionally very similar to ER.
- Controlled Release (CR): A subtype of extended release that delivers drug at a specific, constant, predictable rate. Think osmotic pump systems.
- Delayed Release (DR): Fundamentally different from the others. DR doesn't slow the rate of release. Instead, it delays when release begins, often using an enteric coating to protect the drug from stomach acid so it dissolves in the intestine instead.
ER, XR, XL, SR, and CR all describe the same general concept: slowing drug release over time. DR is the outlier because it delays the start of release rather than controlling the speed.
The distinction between delayed release vs extended release matters clinically. An enteric-coated aspirin (DR) releases its full dose at once, just in the intestine rather than the stomach. An extended release metformin tablet releases its dose gradually across many hours. Same pill bottle shelf, very different pharmacokinetics.
And when patients compare sustained release vs extended release side by side, the functional difference is often negligible. Pharmaceutical references note that sustained release formulations maintain consistent blood concentrations much like ER versions, with the primary distinction being that CR formulations offer more precise rate control than SR. For the patient, the practical experience is nearly identical.
Decoding the Abbreviations on Your Prescription Bottle
Manufacturers choose different suffixes largely for trademark and branding purposes. Wellbutrin alone comes in IR, SR, and XL versions, each using a slightly different release profile, but all three extended-duration forms aim to keep bupropion levels steady. The extended release medical abbreviation you see on your label tells your pharmacist which specific formulation was prescribed, ensuring you get the right product with the right dosing schedule.
Here's a quick reference for the most common abbreviations you'll encounter:
| Abbreviation | Full Term | What It Means for You | Example Context |
|---|---|---|---|
| IR | Immediate Release | Fast-acting; may need multiple doses per day | Acute pain relief, breakthrough symptoms |
| ER | Extended Release | Slow release over 8-24 hours; fewer daily doses | Metformin ER for diabetes management |
| XR | Extended Release | Same as ER; different brand naming | Effexor XR for depression and anxiety |
| XL | Extended Release | Same as ER; typically once-daily dosing | Wellbutrin XL for depression |
| SR | Sustained Release | Gradual release; usually twice-daily dosing | Wellbutrin SR for depression |
| CR | Controlled Release | Precise, constant release rate; once daily | Paxil CR for anxiety disorders |
| DR | Delayed Release | Release starts later (intestine, not stomach) | Enteric-coated aspirin, omeprazole DR |
| LA | Long-Acting | Extended duration of effect | Verapamil LA for blood pressure |
| CD | Controlled Delivery | Engineered release profile; once daily | Diltiazem CD for hypertension |
The xr medical abbreviation and the sr medical abbreviation both appear frequently when you see er on prescription labels for the same drug available in multiple formulations. Don't assume that XR is "better" than SR or that CR is more advanced than ER. Your doctor selects the specific formulation based on your condition, the drug's pharmacokinetics, and how many times per day you can realistically take a pill.
What truly matters isn't which two letters follow the drug name. It's that you take the exact formulation prescribed, at the dose and frequency your doctor specified. Swapping between an SR and an XL version of the same drug without medical guidance can alter your blood levels significantly, because the release profiles, while conceptually similar, aren't always interchangeable. That sensitivity to formulation details is also why these tablets come with strict rules about how you handle and swallow them.

Safety Rules Every ER Tablet User Should Know
Knowing which letters appear on your bottle is one thing. Knowing how to handle what's inside is another entirely. Extended release medication comes with handling rules that don't apply to standard pills, and breaking those rules can turn a safe, therapeutic dose into a dangerous one.
Dose Dumping and Why Crushing ER Tablets Is Dangerous
Here's the scenario pharmacists worry about most: a patient has trouble swallowing, so they crush their extended release pills or try to figure out how to open a capsule pill to mix the contents with food. With an immediate release medication, that might be fine. With an ER formulation, it can be life-threatening.
The phenomenon is called dose dumping. When you crush, chew, or break apart time release pills, you destroy the physical structure that controls how do extended release pills work. The matrix, membrane, or coating that was designed to meter out medication over 12 to 24 hours is gone. The entire dose floods your bloodstream at once, producing plasma concentrations that can spike well above the toxic threshold.
Consider a morphine extended-release tablet (MS Contin) prescribed at 60 mg every 12 hours. That's 60 mg engineered to release gradually. Crush it, and you've created the equivalent of a massive immediate-release dose hitting your system in minutes. Clinical guidance from Enclara Pharmacia lists dose dumping and increased toxicity as the primary risks of manipulating modified-release dosage forms, noting that this applies across all extended-release types including ER, XR, XL, SR, LA, CR, and CD formulations.
The same logic applies to patients wondering how to open a pill capsule containing coated beads. Some extended release capsules are specifically designed to be opened and sprinkled on applesauce, and their prescribing information will say so explicitly. Others contain beads with precise coatings that must not be chewed or crushed. The only safe way to know how to take a capsule pill correctly is to check the product labeling or ask your pharmacist.
What about splitting? The FDA states that most sustained, controlled, or timed release medications are not meant for splitting. In rare cases where splitting is approved, the tablet will be scored and the labeling will explicitly confirm it's safe. Some matrix-type tablets have uniform drug distribution throughout, making time release pills split in half a viable option, but only when the manufacturer has validated this. Never assume a score line means it's safe to split an ER tablet.
Here are the essential do's and don'ts for taking extended release medication safely:
- Do swallow ER tablets whole with a full glass of water.
- Do check your label for food requirements. Some ER formulations must be taken with food to ensure proper absorption; others should be taken on an empty stomach.
- Do ask your pharmacist before splitting any scored ER tablet.
- Do take your dose at the same time each day to maintain steady blood levels.
- Don't crush, chew, or break extended release pills unless your pharmacist explicitly confirms it's safe.
- Don't attempt to open a pill capsule marked as extended release without checking the prescribing information first.
- Don't dissolve ER tablets in water or other liquids before swallowing.
- Don't take ER medications with alcohol, which can accelerate drug release from some formulations and trigger dose dumping.
Missed Doses and Switching Between IR and ER Safely
What happens if you forget a dose of your extended release medication? The instinct to double up on the next dose is understandable but dangerous. Taking two ER doses close together can push your blood levels above the therapeutic window, essentially creating the same overdose risk as dose dumping.
NHS Specialist Pharmacy Service guidance offers a practical framework: if your dose is less than two hours late, take it as soon as you remember. If it's significantly past due, skip the missed dose and resume your normal schedule. Never take a double dose to compensate. For high-risk medications like antiseizure drugs or Parkinson's treatments, even a short delay can have clinical consequences, so contact your prescriber if you're unsure.
Switching between IR and ER versions of the same drug is another area where patients sometimes run into trouble. You might assume that 500 mg of a drug is 500 mg regardless of the formulation. But the total daily dose, dosing frequency, and peak blood levels all change when you move between release types. A patient taking 250 mg IR three times daily (750 mg total) might switch to a single 750 mg ER tablet, but the pharmacokinetic profile is completely different. Your doctor needs to recalculate the dose, adjust the timing, and monitor your response during the transition.
The bottom line: extended release pills are engineered with precision, and they need to be taken with equal precision. The same technology that makes them effective for 12 to 24 hours also makes them unforgiving when mishandled. Your pharmacist is your best resource for any questions about crushing, splitting, missed doses, or formulation switches.
These safety considerations aren't abstract. They play out daily across some of the most commonly prescribed medication categories in modern medicine, where ER formulations have become the standard of care for millions of patients managing chronic conditions.
Real-World Medications That Use Extended Release Technology
Walk into any pharmacy and you'll find extended release formulations lining the shelves across nearly every therapeutic category. These aren't rare specialty drugs. They're some of the most widely prescribed medications in the world, chosen specifically because their active ingredients benefit from slow, steady delivery.
Common Medications That Use Extended Release
Each extended release example below represents a drug category where the ER formulation solves a specific clinical problem, whether that's a short half-life, dose-related side effects, or the need for round-the-clock symptom control.
- Diabetes management: Metformin ER (Glucophage XR) is one of the most prescribed time release medications in the world. The immediate release version commonly causes gastrointestinal side effects like nausea and diarrhea. The ER formulation reduces these local GI effects by releasing the drug gradually along the intestinal tract rather than dumping it all in the stomach.
- Cardiovascular drugs: Metoprolol succinate (Toprol XL) and verapamil are classic examples. If you've ever wondered about verapamil SR vs ER, both are extended-duration formulations designed to maintain steady blood pressure control over 24 hours. Without the sustained release format, patients would need multiple daily doses to prevent dangerous blood pressure fluctuations.
- Pain management: The Tylenol ER pill (acetaminophen extended release) delivers 650 mg over 8 hours rather than requiring a new dose every 4 to 6 hours. What is Tylenol ER in practical terms? It's the same active ingredient as regular Tylenol, just engineered to release more slowly so patients with chronic pain get longer-lasting relief from fewer tablets. Prescription opioid ER formulations like morphine sulfate ER serve a similar purpose for severe pain.
- Mental health: Bupropion (Wellbutrin XL), venlafaxine (Effexor XR), and quetiapine (Seroquel XR) all use extended release technology. Clinical evidence shows that bupropion in immediate release form at high single doses increases seizure risk due to blood level spikes. The XL formulation allows a full 300 mg daily dose to be given safely as a single tablet by blunting that peak concentration.
- ADHD: Methylphenidate OROS (Concerta) uses osmotic pump technology to deliver medication steadily throughout the school and work day. Without ER, children would need a midday dose at school, creating compliance and stigma issues.
- Cough and cold: Guaifenesin ER (Mucinex) is an over-the-counter extended release example that keeps the expectorant working for 12 hours instead of requiring doses every 4 hours.
Why Doctors Choose ER Over IR for Certain Conditions
Two main pharmacological factors drive the decision to prescribe a sustained release medication over its immediate release counterpart.
The first is half-life. Drugs that leave the body quickly need frequent redosing to stay within the therapeutic window. Buspirone, for instance, has such a short half-life that it requires two to three daily doses in IR form. An extended release version consolidates that into a single daily tablet. The same logic applies to carbamazepine, where a short half-life means that without ER formulation, blood levels can drop low enough between doses to trigger breakthrough seizures.
The second factor is peak-related side effects. Some drugs cause problems not because of total daily exposure, but because of how high blood levels spike after each dose. Bupropion's seizure risk, quetiapine's sedation, and metformin's GI distress are all concentration-dependent. Flattening the peak with time release medication technology reduces these effects without reducing efficacy.
The clinical situation matters too. A patient recovering from surgery may need fast-acting IR pain relief that can be titrated hour by hour. A patient managing chronic arthritis benefits from steady, all-day coverage with an ER formulation. Acute conditions favor speed. Chronic conditions favor stability.
This interplay between drug properties and patient needs is what makes formulation science so consequential. The same molecule can behave like two different medications depending on how it's packaged, and that packaging requires serious engineering precision to get right.

How Extended Release Tablets Are Formulated and Manufactured
That engineering precision doesn't happen by accident. Turning a drug molecule into a reliable extended release tablet requires a manufacturing process far more complex than pressing powder into a disc. Every polymer choice, every coating thickness, and every compression parameter must be calibrated so the tablet performs identically whether it's the first unit off the line or the millionth.
The Science Behind Manufacturing ER Tablets
Manufacturing an extended release tablet starts long before anything touches a tablet press. During pre-formulation, scientists select polymers based on the drug's solubility, the desired release duration, and how the tablet will behave in varying GI conditions. Hydroxypropyl methylcellulose (HPMC) might be chosen for a hydrophilic matrix system, while ethylcellulose could serve as a rate-controlling membrane for a sustained release capsule or an osmotic pump design. For a delayed release capsule intended to bypass the stomach entirely, enteric polymers like methacrylic acid copolymers are layered to resist acidic pH.
Industry experts at Colorcon identify four primary challenges in extended-release tablet formulation: achieving the target release profile, maintaining batch-to-batch consistency, matching innovator products for generic equivalence, and bridging technical expertise gaps that many manufacturers face internally.
Here are the key manufacturing considerations that determine whether an extended release tab will perform as designed:
- Polymer selection and grade: Different viscosity grades of the same polymer produce dramatically different gel layers and diffusion rates. A slight change in HPMC grade can shift a 12-hour release profile to 8 hours.
- Granulation and blending uniformity: The drug and excipients must be distributed evenly throughout the blend. Segregation during mixing leads to tablets with inconsistent drug content and unpredictable time release behavior.
- Compression parameters: Tablet density and porosity are locked in during compression. Too much force can damage functional coatings on multiparticulate beads. Too little creates porous tablets that release drug too quickly.
- Coating precision: For coated systems, film thickness must be uniform across every tablet. A variation of even a few microns can alter dissolution timing, especially in osmotic pump designs where the membrane controls water ingress.
- Dissolution testing and IVIVC: Every batch undergoes dissolution testing to verify the release curve matches the target profile. Establishing an In Vitro-In Vivo Correlation (IVIVC) links lab results to real-world blood levels, reducing the need for repeated human studies during scale-up.
The production realities of extended-release tablets mean that even a well-designed formulation can fail at scale if equipment isn't up to the task. Weight variation, capping defects, and inconsistent coating all show up as dissolution failures during quality control, and regulators hold manufacturers to tight specifications under SUPAC guidelines for any post-approval changes.
Working with OEM and ODM Partners for Custom Tablet Formulation
Not every brand has the in-house expertise or equipment to develop sustained release tablets from scratch. This is where contract manufacturing partnerships become essential. OEM (Original Equipment Manufacturer) and ODM (Original Design Manufacturer) partners provide the formulation science, production infrastructure, and quality systems that allow brands to bring complex dosage forms to market without building everything internally.
For nutrition brands, supplement companies, and functional food businesses looking to develop specialized tablet or capsule products, partners like ZhuFeng offer customized formulation and scalable production across multiple dosage formats, including hard capsules, tablets, soft capsules, powder and granules, gummy candy, and oral liquids. This flexibility lets brands explore time release and other advanced tablet designs while leveraging established manufacturing capabilities and quality control systems.
Whether the goal is a simple extended release tab for a single ingredient or a multi-layer sustained release tablets design, the right manufacturing partner bridges the gap between formulation concept and commercial-scale reality. The expertise required to produce consistent ER products, from polymer selection through dissolution validation, is exactly the kind of specialized knowledge that OEM/ODM relationships are built to provide.
Manufacturing complexity is one side of the equation. For patients, what matters most is how all of this translates into practical decisions about their daily medication routine.
What This Means for Your Health and Medication Routine
So whats extended release, really? It's physical and chemical engineering working inside a single tablet to keep your blood levels steady, your side effects low, and your dosing schedule simple. Every mechanism covered in this article, from swelling matrices to osmotic pumps to coated bead capsules, exists to solve one problem: keeping medication inside the therapeutic window for as long as possible.
Key Takeaways About Extended Release Technology
Here's what matters most for your daily routine. How does extended release pills work in practice? The tablet controls the rate at which drug molecules reach your bloodstream, spreading a single dose across 12 to 24 hours instead of releasing everything in minutes. That steady delivery is why ER formulations show significantly higher medication adherence than their immediate release counterparts, with studies across 15 chronic medications finding an average 5.4% improvement in adherence among XR users, a margin associated with meaningful clinical outcomes.
The safety rules are non-negotiable: never crush, chew, or split an extended release tablet unless your pharmacist confirms it's safe. Don't double up on missed doses. Don't switch between IR and ER versions without your doctor recalculating the regimen. These aren't suggestions. They're the difference between therapeutic benefit and potential harm.
Making Informed Decisions About Your Medications
Understanding what is extended release mean for your specific prescription puts you in a stronger position during conversations with your healthcare team. You can ask informed questions about why a particular formulation was chosen, whether a ghost shell is expected, or how food affects absorption.
Advances in tablet formulation continue pushing the field forward, with newer polymer systems and manufacturing techniques enabling even more precise release profiles. For businesses interested in developing their own tablet or capsule products, OEM/ODM manufacturing partners like ZhuFeng offer customized formulation support across multiple dosage formats to bring these concepts from lab to shelf.
The entire purpose of extended release technology is to keep your medication within the therapeutic window, above the minimum effective dose and below the toxic threshold, for as long as possible with as few pills as possible.
What is a time release pill if not a small feat of engineering designed to make your life easier and your treatment safer? Now that you understand how does extended release work at every level, from polymer chemistry to plasma curves, you're equipped to follow your medication instructions with confidence and clarity.
Frequently Asked Questions About Extended Release Tablets
1. What happens if you crush or chew an extended release tablet?
Crushing or chewing an ER tablet destroys the physical structure controlling drug release, causing dose dumping. The entire dose meant for 12 to 24 hours floods your bloodstream at once, potentially pushing blood levels into the toxic range. This can cause dangerous overdose symptoms. Always swallow ER tablets whole with water unless your pharmacist explicitly confirms an alternative method is safe for your specific medication.
2. How long does it take for an extended release tablet to start working?
Extended release tablets typically begin releasing medication within 30 minutes to 2 hours after swallowing, once stomach acid starts working on the outer coating. However, peak therapeutic effect takes longer to achieve compared to immediate release versions because the drug is released gradually. The full transit from swallowing to complete absorption spans 12 to 24 hours depending on the formulation type, with drug entering your bloodstream continuously throughout that period.
3. Is there a difference between extended release and sustained release medications?
Functionally, extended release (ER) and sustained release (SR) medications are very similar. Both are designed to release drug slowly over many hours to maintain steady blood levels. The primary distinction is that controlled release (CR) formulations offer more precise rate control than SR versions. Manufacturers often choose different abbreviations for branding purposes rather than because the mechanisms are fundamentally different. However, you should never swap between ER and SR versions of the same drug without your doctor's guidance, as their specific release profiles may not be identical.
4. Why do I see a whole pill in my stool after taking extended release medication?
This is called the ghost pill phenomenon and is completely normal for certain ER medications, particularly those using osmotic pump technology. The tablet has a rigid, insoluble outer shell with a tiny laser-drilled hole. Water enters the shell by osmotic pressure and pushes the dissolved drug out through the hole. Once all medication has been expelled and absorbed into your bloodstream, the empty shell passes through your digestive system intact. Medications like Concerta and Invega commonly produce these ghost shells.
5. Can you split extended release tablets in half?
Most extended release tablets should not be split, as doing so can compromise the release mechanism and cause dose dumping. However, some scored ER tablets with uniform matrix designs are specifically validated for splitting by the manufacturer. The FDA advises that sustained, controlled, or timed release medications are generally not meant for splitting. Only split an ER tablet if the prescribing information explicitly states it is safe and your pharmacist confirms it. A score line alone does not guarantee safe splitting.


