

Why You Should Never Crush Extended Release Tablets
The Short Answer About Crushing ER Tablets
Can you crush extended release tablets? No. Unless a pharmacist or prescriber has specifically told you it is safe, crushing pills that carry an extended-release designation can be dangerous and even fatal. The physical structure of these tablets IS the delivery system. When you destroy that structure, you destroy the mechanism that controls how much drug enters your bloodstream and how fast it gets there.
The result is a phenomenon called dose dumping, where a medication designed to release gradually over 12 to 24 hours floods your system all at once. That means you receive the full dose in minutes instead of hours, pushing drug levels into toxic territory.
Dose dumping from a crushed extended-release tablet can release an entire day's worth of medication into your body within minutes, potentially causing overdose, organ damage, or death.
This is not a theoretical risk. The FDA pulled the extended-release opioid Palladone from the market after it demonstrated dangerous dose-dumping effects that could prove lethal. Crushing any ER tablet creates a similar scenario by bypassing the built-in safety controls entirely.
Why This Question Matters for Your Safety
People search this question for real, practical reasons. Maybe you struggle with swallowing large tablets. Maybe you are a caregiver helping an elderly parent in hospice who can no longer take pills whole. Maybe your child needs a medication that only comes in tablet form, or you are administering drugs through a feeding tube. These are legitimate situations, and they deserve safe solutions rather than risky workarounds.
The do not crush list maintained by the Institute for Safe Medication Practices (ISMP) contains hundreds of medications that should never be altered. If you are wondering what are 3 medications that cannot be crushed, consider morphine sulfate ER (MS Contin), oxycodone ER (OxyContin), and bupropion XL (Wellbutrin XL). These represent just a fraction of the 5 drugs that should never be crushed and the many others on that list where crushing pills could trigger serious harm.
And for a common question like can you crush Tylenol: standard immediate-release Tylenol tablets can generally be crushed safely, but Tylenol 8HR (acetaminophen ER) cannot because it uses a modified-release formulation. That single distinction between immediate-release and extended-release versions of the same drug is exactly why checking with your pharmacist matters every time.
The good news is that safer alternatives almost always exist. Liquid formulations, immediate-release versions taken more frequently, patches, and other dosage forms can solve the swallowing problem without putting you at risk. The key is knowing why ER tablets work the way they do and what happens inside your body when that design is compromised.
How Extended Release Tablets Actually Work Inside Your Body
So how do extended release pills work, exactly? The answer comes down to physical engineering at a tiny scale. Each time release pill is a miniature drug-delivery device, and its shape, layers, and internal structure control precisely how much medication reaches your bloodstream each hour. Destroy that structure, and you destroy the schedule.
How Extended Release Technology Controls Your Dose
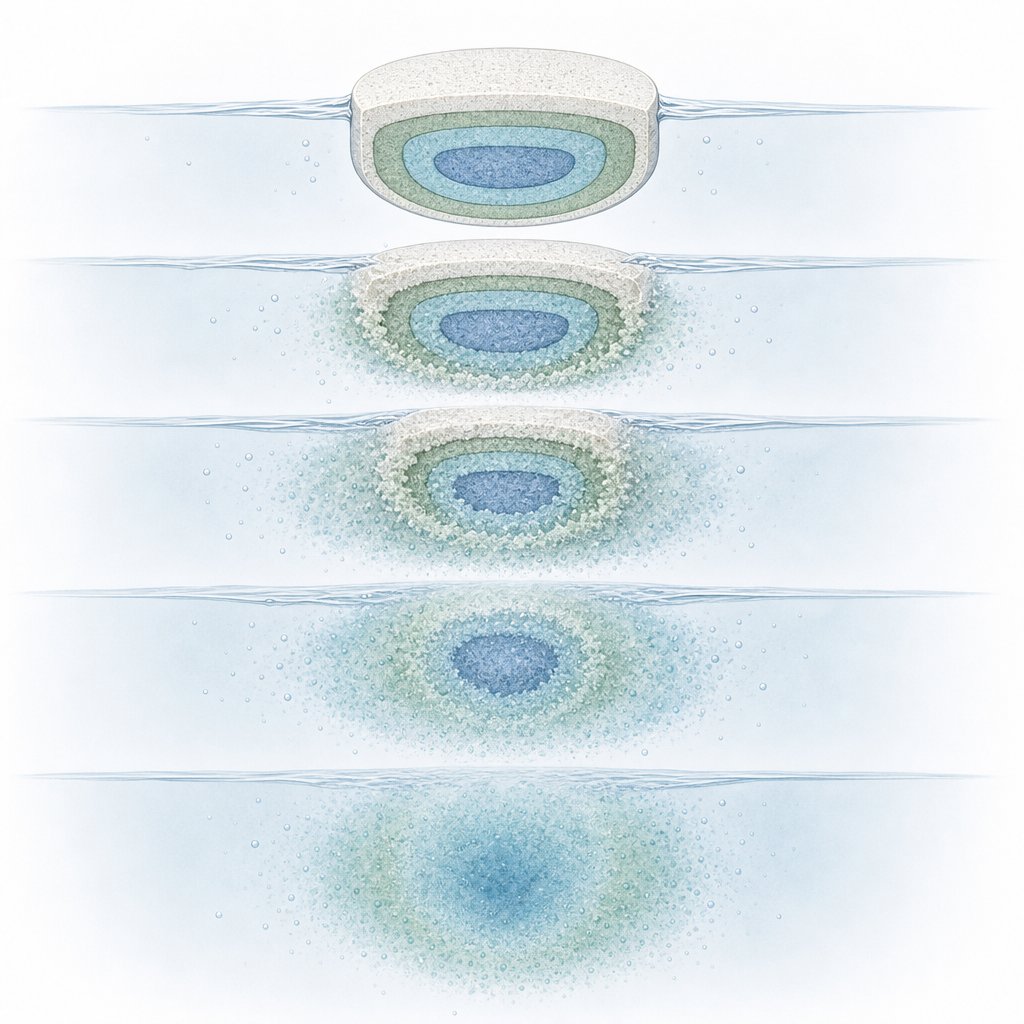
Imagine dropping a sugar cube into a cup of coffee. It does not vanish instantly. It dissolves layer by layer, gradually sweetening the liquid over time. That slow, predictable dissolution is essentially what ER technology replicates inside your digestive tract. Different manufacturers use different engineering approaches, but they all share one principle: the physical structure is the timer.
Here are the four main mechanisms you will find in today's ER medications:
- Hydrophilic matrix systems — The drug is mixed throughout a water-swellable polymer scaffold. When the tablet contacts stomach fluid, the outer layer forms a gel barrier. Medication can only escape by slowly diffusing through that gel or as the gel gradually erodes. Think of it like a sponge releasing soap only as fast as water can seep through its pores. According to pharmaceutical research, polymer type and concentration are adjusted to make release faster or slower as needed.
- Osmotic pump systems (OROS) — A tablet core is surrounded by a semi-permeable membrane with a laser-drilled hole. When you place these pills in water (your stomach fluid), water passes through the membrane, dissolves the drug inside, and builds pressure that pushes a steady stream of drug solution out through the tiny orifice. The release rate stays remarkably constant regardless of food or pH changes in your gut.
- Coated pellet (multi-particulate) systems — Instead of one solid tablet, the capsule contains hundreds of tiny beads. Each bead has a polymer coating of a different thickness. Thin-coated beads dissolve first, thicker ones dissolve hours later. The result is staggered waves of drug release across 12 to 24 hours. How long does it take pills to dissolve in this format? Individual pellets may release over a span of 1 to 20 hours depending on their coating layer.
- Wax or insoluble matrix systems — Drug particles are embedded in a waxy or inert polymer framework that does not dissolve at all. Instead, fluid seeps into tiny channels within the matrix and slowly leaches the drug out, much like water trickling through packed sand. The empty shell often passes intact in stool as a harmless "ghost tablet."
What Happens When You Destroy the Release Mechanism
When a tablet is crushed into powder, every one of these systems fails immediately and completely. There is no gel barrier left to slow diffusion. No membrane to regulate osmotic flow. No intact coatings to stagger pellet release. No wax channels to limit drug escape. The entire dose, meant to sustain you for half a day or longer, becomes available for absorption within minutes.
People sometimes search how to pulverize pills for easier swallowing, not realizing that with ER formulations, pulverizing is functionally the same as taking multiple doses at once. A 24-hour oxycodone ER tablet crushed into fine powder delivers its full payload as if it were an immediate-release mega-dose. The same logic applies if you wonder whether you can you crush sustained release tablets of any class: the answer remains no, because the structure you are destroying is not packaging. It is the medicine's safety mechanism.
This engineering reality is why identifying ER tablets before you ever reach for a pill crusher matters so much. The clues are right there on your prescription label, if you know what to look for.
How to Identify Extended Release Tablets by Their Labels
Your prescription label holds the clues. Every extended-release tablet carries a suffix, a short abbreviation tacked onto the drug name, that signals its release mechanism. Recognizing these suffixes is the fastest way to determine whether a tablet belongs on the do not crush list before you ever consider altering it.
Decoding ER Tablet Suffixes on Your Prescription Label
When you pick up a prescription bottle, look at the drug name closely. You might see something like "metoprolol succinate ER" or "bupropion XL." Those trailing letters are not random. They tell you the tablet uses a modified-release formulation, and that means its physical structure controls how the drug enters your body. Crush it, and you bypass that control entirely.
Here is a reference table covering the most common suffixes you will encounter:
| Suffix | Full Name | Meaning | Example Context |
|---|---|---|---|
| ER | Extended Release | Drug releases gradually over an extended period, typically 12-24 hours | Metformin ER (Glumetza), Acetaminophen ER (Tylenol 8HR) |
| XR | Extended Release | Same concept as ER; alternate branding used by some manufacturers | Quetiapine XR (Seroquel XR), Venlafaxine XR (Effexor XR) |
| SR | Sustained Release | Prolongs drug release from the tablet so levels remain therapeutic longer | Bupropion SR (Wellbutrin SR), Propafenone SR (Rythmol SR) |
| CR | Controlled Release | Releases drug at a specific, constant rate to maintain steady blood levels | Zolpidem CR (Ambien CR), Paroxetine CR (Paxil CR) |
| LA | Long Acting | Formulated to maintain effects over a prolonged duration between doses | Diltiazem LA (Cardizem LA), Propranolol LA (Inderal LA) |
| CD | Controlled Delivery | Uses multi-particulate beads or specialized matrix for timed drug delivery | Diltiazem CD (Cardizem CD), Methylphenidate CD (Metadate CD) |
| XL | Extended Length | Designed for once-daily dosing by extending the release window to 24 hours | Bupropion XL (Wellbutrin XL), Nifedipine XL (Procardia XL) |
| SA | Sustained Action | Older designation indicating a slow-release formulation | Less common today; seen in some legacy formulations |
The rule of thumb is simple: if you see any of these suffixes on your medication label, assume the tablet is on the do not crush medication list unless your pharmacist explicitly confirms otherwise. Many healthcare facilities keep a do not crush list PDF from resources like the ISMP or EMPR posted in their medication rooms for exactly this reason.
Enteric Coated and Other Do-Not-Crush Designations
Extended-release suffixes are not the only warning signs. Enteric-coated tablets, marked with "EC" or sometimes labeled "safety-coated," use a special film that prevents the tablet from dissolving in your stomach. Instead, the coating holds until the tablet reaches the small intestine, where the pH triggers dissolution. This protects your stomach lining from irritation and ensures the drug absorbs where it is most effective.
Can enteric coated tablets be crushed? No. Crushing destroys the protective film, exposing the drug to stomach acid prematurely. This can cause significant gastric irritation and reduce the medication's effectiveness. Common examples include aspirin EC (Ecotrin), sulfasalazine DR (Azulfidine EN-Tabs), and bisacodyl (Dulcolax). If you are wondering can you crush enteric coated tablets of any kind, the answer remains the same: the coating exists for a clinical reason, and removing it creates problems.
Beyond ER and EC designations, other medications carry do not crush warnings for different reasons. Hazardous drugs like chemotherapy agents can expose caregivers to toxic powder when altered. Medications using amorphous solid dispersion or nanocrystal technology lose their bioavailability if the tablet structure is compromised. And sublingual or buccal formulations need to dissolve in the mouth, not the stomach, so crushing and swallowing defeats their purpose entirely.
A practical tip: scored tablets, those with a visible line down the middle, are generally designed to be split in half for dose adjustment. If your tablet has a score line, that is a clue it may appear on a list of medications that can be split safely. However, a score line does not mean the tablet can be crushed into powder. Splitting and crushing are two very different actions with very different consequences, especially for modified-release formulations.
When in doubt, your pharmacist can cross-reference your specific medication against the complete do not crush medication list and tell you whether splitting, crushing, or any other alteration is safe. That 30-second conversation could prevent a serious adverse event, particularly with the high-risk drug classes covered next.
Common Extended Release Medications You Should Never Crush
Knowing the suffixes is one thing. Recognizing your own medication on a do-not-crush list is another. Patients often search for their specific drug name because they need a concrete answer, not a general rule. Below, you will find common ER medications grouped by therapeutic category so you can quickly locate yours and understand why altering it is dangerous.
Common ER Medications by Therapeutic Category
This table covers frequently prescribed extended-release formulations across major drug classes. Each category carries its own set of risks if the controlled-release mechanism is destroyed.
| Category | Common ER Medications | Why Crushing Is Dangerous |
|---|---|---|
| Pain (Opioids) | Oxycodone ER (OxyContin), Morphine sulfate ER (MS Contin), Hydromorphone ER (Exalgo), Oxymorphone ER (Opana ER) | Dose dumping delivers a potentially fatal opioid load, causing respiratory depression, coma, or death within minutes |
| Cardiovascular | Metoprolol succinate ER (Toprol-XL), Nifedipine ER (Procardia XL), Diltiazem ER (Cardizem LA/CD), Verapamil ER (Calan SR) | Sudden release can trigger severe hypotension, dangerously slow heart rate, or cardiac arrest |
| Psychiatric | Quetiapine XR (Seroquel XR), Bupropion XL (Wellbutrin XL), Venlafaxine XR (Effexor XR), Paroxetine CR (Paxil CR) | Rapid absorption causes extreme sedation, seizure risk (bupropion), or serotonin-related toxicity |
| Diabetes | Metformin ER (Glumetza, Fortamet) | Immediate release of the full dose causes severe gastrointestinal distress and increases lactic acidosis risk |
| Neurological | Levetiracetam ER (Keppra XR), Carbidopa-levodopa ER (Sinemet CR), Carbamazepine ER (Tegretol-XR) | Dose dumping leads to excessive sedation, dizziness, ataxia, or toxic drug levels that provoke the very seizures the medication is meant to prevent |
| Respiratory / Other | Theophylline ER (Theo-24), Guaifenesin ER (Mucinex), Potassium chloride ER (Klor-Con) | Theophylline toxicity causes seizures and arrhythmias; potassium dumping can trigger fatal cardiac events; guaifenesin overload causes severe nausea |
A few of these deserve extra attention because they generate frequent patient questions. Can quetiapine be crushed? Not the XR formulation. Seroquel XR uses a matrix system designed for once-daily dosing, and crushing it releases the entire dose immediately, causing profound sedation and a dangerous blood pressure drop. The immediate-release version of quetiapine (regular Seroquel) can typically be crushed, but you must confirm with your pharmacist which version you have.
Similarly, people often ask whether metformin can be crushed. Standard immediate-release metformin tablets are generally safe to crush, but metformin ER (Glumetza, Fortamet) absolutely cannot be. The ER version uses a polymer matrix that slowly releases the drug to minimize the gastrointestinal side effects metformin is notorious for. Crush it, and you get the full dose hitting your stomach at once, along with the nausea, cramping, and diarrhea the ER design was built to prevent.
Can levetiracetam be crushed? Again, it depends on the formulation. Immediate-release levetiracetam (Keppra) tablets can usually be crushed or split, and a liquid formulation exists. But Keppra XR is a different product with a different release profile, and crushing it eliminates the extended-release mechanism that maintains steady anti-seizure drug levels throughout the day.
Using the ISMP Do-Not-Crush List as Your Reference
The most comprehensive professional resource for this topic is the ISMP do-not-crush list, formally titled "Oral Dosage Forms That Should Not Be Crushed." Maintained by the Institute for Safe Medication Practices, this medication do not crush list catalogs hundreds of oral dosage forms along with the specific reason each one should remain intact. Hospitals, long-term care facilities, and pharmacies across the United States use it as their go-to reference when questions arise about altering a tablet.
The ISMP do not crush list is updated periodically to reflect new drug approvals and reformulations. It includes not only extended-release products but also enteric-coated medications, hazardous drugs, and formulations with specialized absorption technology. Many facilities keep a printed version, sometimes formatted as a do not crush list ISMP quick-reference card, posted in medication preparation areas.
A few important points about using this resource:
- The list covers brand and generic names, so you can search by either.
- It specifies the reason for the do-not-crush designation (slow release, enteric coating, hazardous substance, etc.), which helps clinicians identify safe alternatives.
- It is not a static document. New ER formulations enter the market regularly, so always verify against the most current version.
- Your pharmacist has access to the complete, updated list and can cross-reference your specific medication in seconds.
Keep in mind that the table above and the ISMP list are not exhaustive. New extended-release products reach pharmacies every year, and generic manufacturers sometimes use different release technologies than the original brand. The safest approach is always the same: if you are unsure whether your tablet can be altered, ask your pharmacist before reaching for a pill crusher. That single question becomes especially critical when the medication falls into a high-risk category where dose dumping does not just cause discomfort but threatens your life.
Understanding Which Crushed ER Tablets Pose the Greatest Danger
Not every crushed ER tablet carries the same consequences. While the rule is universal — do not crush any extended-release formulation without professional guidance — the reality is that some medications will send you to the emergency room and others will leave you with a bad stomachache. Understanding where your medication falls on that spectrum helps you grasp the urgency of the warning.
Risk Levels When ER Tablets Are Crushed
Think of this as a danger tier list. Every ER tablet on it should remain intact, but the stakes escalate dramatically depending on the drug class involved.
- High risk (potentially fatal): Opioid ER formulations top this tier. Crushing oxycodone ER or morphine sulfate ER releases a dose designed for 12 to 24 hours into your bloodstream within minutes. The result is respiratory depression — your brain literally stops telling your lungs to breathe. Cardiovascular ER drugs sit in this same tier. Can metoprolol be crushed? Not the ER version (Toprol-XL). Sudden release of a full day's beta-blocker dose can crash your heart rate and blood pressure to dangerous lows, potentially triggering cardiac arrest. Nifedipine ER and diltiazem ER carry similar risks of acute hypotensive crisis.
- Moderate risk (serious but less likely to be immediately fatal): Psychiatric ER medications fall here. Can Seroquel be crushed? The XR formulation cannot. Crushing quetiapine XR dumps the entire dose at once, causing profound sedation, orthostatic hypotension, and in some cases dangerous QT prolongation. Bupropion XL is another concern — its ER design exists partly because immediate-release bupropion at high single doses raises seizure risk significantly. Venlafaxine XR crushed can trigger serotonin-related toxicity and severe discontinuation-like symptoms from erratic blood levels.
- Lower risk (harmful but typically not life-threatening): Some supplement and vitamin ER formulations sit in this tier. Can you crush potassium pills in extended-release form? You should not. Why can't you crush potassium pills? Because concentrated potassium released all at once causes severe gastrointestinal ulceration and irritation. MyHealth Alberta notes that crushing or chewing potassium ER tablets "can release all of the drug at once, increasing the risk of side effects," including stomach ulcers and GI bleeding. Can potassium tablets be crushed if they are the dispersible type? Some potassium formulations (like K-Dur dispersible tablets) can be dissolved in water as directed, but standard wax-matrix potassium ER tablets cannot be crushed. Guaifenesin ER (Mucinex) is another lower-tier example — crushing it causes nausea and GI upset rather than a life-threatening event, though it still defeats the purpose of the extended-release design. Similarly, iron supplement ER formulations cause intense stomach irritation when their protective structure is destroyed.
The key takeaway: "lower risk" does not mean "safe to crush." It means the margin between discomfort and a medical emergency is wider. Every tier still warrants a call to your pharmacist before altering the tablet.
Crushing vs Splitting vs Chewing an ER Tablet
People sometimes assume that splitting a tablet in half is less harmful than grinding it to powder, or that chewing is somewhere in between. All three actions compromise the release mechanism, but the degree of damage differs.
- Crushing — Complete destruction. The tablet becomes fine powder with maximum surface area exposed. Drug release is immediate and total. This is the worst-case scenario for dose dumping.
- Splitting — Partial destruction. Breaking an ER tablet in half exposes the internal matrix at the break point, allowing faster drug release from that surface. Some matrix tablets may still provide partially controlled release from the intact portions, but the designed release profile is compromised. You cannot predict how much drug will dump early.
- Chewing — Variable destruction. What happens if you chew a pill with an ER formulation? Your teeth fragment the tablet into irregular pieces, dramatically increasing surface area and destroying coating integrity. The result is unpredictable — somewhere between splitting and full crushing depending on how thoroughly you chew. Can you chew pills that are extended-release? No. Even brief chewing breaks enough of the structure to cause significant dose acceleration.
For osmotic pump tablets (like some nifedipine ER products), even splitting in half is catastrophic because the entire system depends on an intact membrane with a single laser-drilled exit hole. Break that membrane anywhere, and the controlled-release mechanism ceases to exist entirely.
For coated-pellet capsules, the situation is slightly different. If you can open the capsule and swallow the intact pellets without chewing, the individual bead coatings may still function. This is why some ER capsules — like Diltiazem CD or Metadate CD — are approved for sprinkling on applesauce. But this only works if the pellets themselves remain unchewed and unground. The moment you crush those beads, you are back to full dose dumping.
The practical lesson here is straightforward: do not assume that a gentler form of alteration is a safe compromise. Whether you crush, split, or chew an ER tablet, you are gambling with a delivery system that was engineered to protect you from the drug's full force hitting your body at once. The severity of that gamble depends on which risk tier your medication occupies — and for high-tier drugs, the consequences can arrive faster than an ambulance.

Safe Alternatives When Swallowing Extended Release Tablets Is Not Possible
Knowing the risks of crushing ER tablets is only half the equation. The other half is solving the actual problem: your patient, your parent, or you physically cannot swallow the tablet whole. This is not a rare situation. Millions of people face it daily, and the solution is never to reach for a pill crusher and hope for the best.
If you are wondering how to take pills if you can't swallow them, the answer starts with understanding that nearly every ER medication has a safer alternative pathway. Your pharmacist or prescriber can identify one, often within the same appointment.
Alternatives for Patients Who Cannot Swallow Whole Tablets
The scenarios driving this challenge are varied, but the solutions overlap significantly:
- Dysphagia (swallowing disorders) — Patients recovering from stroke, living with neurological conditions like Parkinson's disease, or dealing with head and neck cancers often cannot safely take pills. Dry swallowing pills is already risky for these patients, and attempting to swallow a large ER tablet can cause choking or aspiration. Alternatives include liquid formulations (metformin, gabapentin, fluoxetine, and levothyroxine all come in oral liquid versions), transdermal patches, or switching to an immediate-release version given at shorter intervals.
- Pediatric patients — Children often cannot take pills at all, let alone large extended-release tablets. How do you take a capsule when you are six years old? In many cases, you don't. Chewable tablets, oral suspensions, and sprinkle capsules (from the list of capsules that can be opened and mixed with soft food) provide age-appropriate options. Some ER capsules like Metadate CD are specifically approved for opening and sprinkling onto applesauce without chewing the beads.
- Feeding tube administration — Memorial Sloan Kettering states clearly that tablets which are enteric-coated, extended-release, or slow-release "cannot be taken through your feeding tube." The medication must be converted to a liquid form or replaced with an alternative that can be safely dissolved and flushed through the tube without clogging or dose dumping.
- Elderly patients in hospice or long-term care — Hospice medications often need reformulation as patients lose the ability to swallow. Sublingual medication examples include fentanyl (Abstral), ondansetron ODT, and lorazepam concentrate, all of which dissolve under the tongue without requiring the patient to swallow anything. Suppository forms of acetaminophen, morphine, and anti-nausea drugs provide another route entirely.
The NHS Specialist Pharmacy Service maintains an entire guidance series on medicines suitable for adults with swallowing difficulties, covering drug classes from ACE inhibitors to statins. Each entry identifies licensed alternatives, whether tablets can be dispersed in water, and when switching to a different medication within the same class is the safest path.
Caregiver Guidance for Hospice and Elderly Care Settings
If you are a caregiver facing this situation right now, here is a step-by-step decision pathway to follow:
- Stop and do not alter the tablet. Resist the urge to crush, split, or dissolve the ER medication. The risk of harm outweighs the inconvenience of a phone call.
- Contact the prescriber or pharmacist. Explain that the patient can no longer take pills whole. Ask specifically: "Is there a liquid, patch, sublingual, or immediate-release version of this medication?"
- Ask about approved sprinkle methods. Some ER capsules can be opened and their contents sprinkled on soft food without crushing the internal beads. Your pharmacist can check whether your specific medication is on the list of capsules that can be opened safely.
- Request a compounded preparation if needed. If no commercial alternative exists, a compounding pharmacy can often prepare a custom liquid or suspension. These are not FDA-approved products, but they can be a practical solution when standard options fall short.
- Discuss whether the medication is still necessary. In hospice and palliative care settings, deprescribing — stopping medications that no longer serve the patient's comfort goals — is a valid and often overlooked option. A medication that cannot be safely administered may no longer be appropriate for the care plan.
- Document the change. Whatever alternative is chosen, update the medication schedule and communicate the change to every member of the care team. This prevents a future caregiver from accidentally reverting to the original ER tablet.
For anyone struggling with how to take a large pill, simpler techniques can sometimes help with non-ER medications: tilting the chin slightly forward while swallowing, using a thicker liquid like a smoothie, or trying the "pop-bottle method" where you seal your lips around a flexible water bottle and swallow as you squeeze. These tricks help people take pills that are safe to swallow whole but physically difficult due to size. They do not, however, solve the ER problem — because the issue is not just size but the need to keep the tablet's structure intact throughout the digestive tract.
The reassuring reality is that alternatives almost always exist. Between liquid formulations, patches, sublingual options, suppositories, and compounded preparations, very few clinical situations truly have no workaround. The key is involving your pharmacist early, before anyone makes a dangerous decision out of desperation. That same pharmacist can also guide you on what to do if the damage is already done — a scenario that demands immediate action.
What to Do If You Accidentally Crushed an Extended Release Tablet
Maybe you did not read the label carefully. Maybe a well-meaning caregiver ground up a tablet to mix into applesauce without realizing it was an ER formulation. Maybe you are reading this article after the fact, and the crushed medication has already been swallowed. Whatever the circumstance, the next few minutes matter. Here is exactly what to do.
Immediate Steps If You Already Crushed and Took an ER Tablet
First, do not panic, but do act quickly. Dose dumping from a crushed extended-release tablet can produce symptoms within minutes rather than the hours you might expect from a normal overdose scenario. The entire dose that was meant to release over 12 to 24 hours is now available for immediate absorption.
Follow these steps in order:
- Do not induce vomiting. This is critical. The Utah Poison Control Center confirms that inducing vomiting is no longer recommended because it does not work reliably and can cause additional harm, especially if the person becomes drowsy and chokes on vomit. Syrup of ipecac is outdated and potentially dangerous.
- Identify the medication and dose. Grab the pill bottle or packaging. Note the drug name, strength, and how much was taken. This information is essential for whoever you call next.
- Call Poison Control immediately. In the United States, the number is 1-800-222-1222. The line is staffed 24/7 by pharmacists and toxicology-trained specialists who can assess your specific situation in minutes, completely free of charge.
- Monitor for symptoms while you wait for guidance. Watch for signs specific to the drug class involved (detailed below).
- Do not take another dose. Even if your next scheduled dose is approaching, skip it until you have spoken with Poison Control or your prescriber. Your body has already received the full amount.
U.S. Poison Control: 1-800-222-1222 — free, 24/7, staffed by pharmacists. Call immediately if you or someone else has crushed and swallowed an extended-release tablet. If the person cannot breathe, is unconscious, or is having a seizure, call 911 first.
The timeline is what makes dose dumping so dangerous. With a normal accidental double-dose of an immediate-release medication, symptoms may develop gradually over an hour or more. With a crushed ER tablet, the drug floods your system almost as fast as an intravenous injection would. Pharmaceutical research defines dose dumping as the rapid introduction of a "potentially toxic quantity of the drug into systemic circulation," and notes it can prove fatal for potent drugs with a narrow therapeutic index.
When to Seek Emergency Medical Care
Poison Control can often manage lower-risk situations over the phone, monitoring you with follow-up calls. But certain symptoms demand 911 without hesitation. Call emergency services if you observe any of the following:
- Opioid ER medications (oxycodone ER, morphine ER, hydromorphone ER): Watch for slowed or shallow breathing, blue-tinged lips or fingertips, extreme drowsiness progressing to unresponsiveness, or pinpoint pupils. Can norco be crushed? Standard Norco is an immediate-release combination product, but if someone has crushed any opioid ER formulation, respiratory depression can develop within minutes and become fatal without intervention.
- Cardiovascular ER medications (metoprolol ER, nifedipine ER, diltiazem ER): Watch for dizziness, fainting, dangerously slow pulse, chest pain, or confusion from low blood pressure.
- Psychiatric ER medications (quetiapine XR, bupropion XL, venlafaxine XR): Watch for extreme sedation, seizures, rapid or irregular heartbeat, or inability to stay conscious.
As Mayo Clinic's poisoning first-aid guidance states: if the person is drowsy or unconscious, having difficulty breathing, experiencing seizures, or is uncontrollably agitated, call 911 immediately. Do not attempt to drive them to the hospital yourself, because their condition can deteriorate rapidly in transit.
For lower-risk ER medications, the situation is less urgent but still warrants professional guidance. Can Mucinex be crushed? The extended-release version (Mucinex 12-Hour) should not be, though accidentally doing so is unlikely to cause a life-threatening event. Can i crush Mucinex in its regular immediate-release form? Standard guaifenesin tablets without the ER designation can generally be crushed. If someone has crushed guaifenesin ER, they may experience nausea or stomach upset, but a call to Poison Control will confirm whether home monitoring is sufficient. The same applies to can omeprazole be crushed — the delayed-release capsule should remain intact, but accidental alteration typically causes reduced effectiveness and GI discomfort rather than a medical emergency. Can depakote be crushed? Depakote ER absolutely cannot, as rapid valproic acid release can cause serious CNS depression and liver toxicity. Can you crush guanfacine? The ER version (Intuniv) should never be crushed because sudden release can cause severe hypotension and sedation, particularly dangerous in the pediatric patients who commonly take it.
The bottom line: when in doubt, call. Poison Control exists precisely for these moments, and their experts can tell you within minutes whether you need an ambulance or careful observation at home. That single phone call could be the difference between a scare and a tragedy — and it costs nothing. With the immediate crisis addressed, the smarter long-term move is preventing it from happening again by working with your pharmacist to find a formulation that fits your needs safely.

Questions for Your Pharmacist and Choosing the Right Product Format
Preventing a dose-dumping emergency is far simpler than managing one. The most effective prevention tool you have is a short, focused conversation with your pharmacist — someone who can cross-reference your exact medication, your clinical situation, and the full range of available alternatives in minutes. You do not need to know how to crush a pill safely or how to use a pill crusher correctly if you never need to crush the tablet in the first place.
Questions to Ask Your Pharmacist About Your ER Medication
Before you ever search for the best way to crush a pill or buy a pill grinder, bring this list of questions to your next pharmacy visit. Print it, screenshot it, or just remember the key themes. Each question opens a door to a safer solution:
- Is there an immediate-release version of this medication? Many ER drugs have IR counterparts that can be given in smaller, more frequent doses to achieve the same therapeutic effect without the swallowing challenge.
- Can this medication be compounded into a liquid or suspension? Compounding pharmacies can reformulate many drugs into oral liquids with accurate dosing, especially useful for feeding tube patients.
- Are there alternative dosage forms available? Patches (transdermal), sublingual tablets, dissolvable films, suppositories, and injectable options may exist for your drug class.
- Is my capsule approved for opening and sprinkling? Some ER capsules contain coated pellets that can be sprinkled on soft food without chewing. Your pharmacist can confirm whether yours qualifies.
- What should I do if I accidentally crush or split this tablet? Knowing the emergency protocol in advance — before a mistake happens — gives you and your caregivers a clear action plan.
- Is there a therapeutically equivalent medication in a different class that comes in an easier format? Sometimes switching to a different drug that treats the same condition but comes as a liquid or patch is the simplest path forward.
- Can I use any swallowing aids with this specific tablet? Pill-coating lubricants, specialized cups, or thick liquids may help some patients swallow intact tablets without alteration.
Your pharmacist has access to the complete ISMP do-not-crush list, manufacturer guidelines, and compounding references. That five-minute conversation replaces the guesswork of searching the best way to crush pills online and hoping you picked a safe medication to alter.
How Modern Health Product Formats Address Swallowing Challenges
The swallowing problem extends beyond prescription medications. Many people who struggle with tablets or capsules face the same challenge with daily supplements and functional health products. Imagine you need a daily multivitamin, omega-3, or probiotic but cannot physically swallow a large tablet. Do you skip it entirely? You should not have to.
This is exactly why the supplement and health food industry has moved well beyond the traditional tablet-only model. According to IADSA's dosage form guide, supplements are now available in a wide range of formats specifically because manufacturers recognize that one form does not fit every consumer. Chewable forms, for instance, "are often taken by people who have difficulty swallowing tablets or capsules."
Modern supplement formats designed to eliminate swallowing barriers include:
- Oral liquids — Solutions, syrups, and vials that require no swallowing of solid forms. Ideal for elderly consumers and children.
- Powder and granules — Sachets or stick packs that dissolve in water or sprinkle onto food, delivering precise doses without any pill involved.
- Gummy candy — Chewable, flavored formats that feel nothing like medicine. Popular across all age groups and particularly effective for adherence in people who dislike tablets or capsules.
- Soft capsules (softgels) — Smaller and smoother than standard tablets, with a flexible gelatin shell that slides down more easily.
- Hard capsules — Available in smaller sizes than compressed tablets and can sometimes be opened for sprinkling if the contents are not modified-release.
- Effervescent tablets — Dissolve completely in water before consumption, creating a flavored drink rather than a pill to swallow.
For nutrition brands, supplement importers, and private label sellers, offering this range of formats is not just a convenience play — it is an accessibility requirement. Consumers who cannot swallow standard tablets will simply not buy products that only come in that form. OEM/ODM manufacturers like ZhuFeng provide brands with flexible format options spanning oral liquids, powder/granules, gummy candy, soft capsules, and traditional tablets, enabling health products to reach consumers regardless of their swallowing ability. This kind of manufacturing flexibility means a single formulation can be produced across multiple delivery formats, letting brands serve pediatric, elderly, and dysphagia populations without reformulating from scratch.
The broader point applies whether you are choosing a prescription medication format or a daily supplement: the best way to crush a pill is to never need to crush it at all. When your pharmacist helps you find an ER medication alternative that works for your body, and when supplement brands offer formats beyond rigid tablets, the entire crushing question becomes irrelevant. You get your therapeutic benefit, your body gets the dose it needs at the rate it needs it, and nobody ends up calling Poison Control.
If you take away one thing from this article, let it be this: the question is never really how to crush pills safely when those pills are extended-release. The question is which alternative format delivers the same benefit without the risk. That answer exists for nearly every medication and supplement on the market. Ask your pharmacist. Check your options. And leave the pill crusher in the drawer.
Frequently Asked Questions About Crushing Extended Release Tablets
1. What happens if you accidentally crush an extended release tablet?
Crushing an ER tablet causes dose dumping, releasing 12-24 hours of medication into your body within minutes. This can lead to overdose symptoms including respiratory depression (opioids), dangerous blood pressure drops (cardiovascular drugs), or seizures (psychiatric medications). If this happens, do not induce vomiting. Call U.S. Poison Control at 1-800-222-1222 immediately, identify the medication and dose taken, and monitor for symptoms. Call 911 if the person shows difficulty breathing, loss of consciousness, or seizures.
2. What are 3 medications that cannot be crushed?
Three high-risk medications that should never be crushed include oxycodone ER (OxyContin), which can cause fatal respiratory depression from dose dumping; metoprolol succinate ER (Toprol-XL), which can trigger cardiac arrest from sudden blood pressure and heart rate drops; and bupropion XL (Wellbutrin XL), which significantly raises seizure risk when the full dose is released at once. The ISMP do-not-crush list contains hundreds more, and your pharmacist can verify whether your specific medication is safe to alter.
3. How can you tell if a tablet is extended release?
Look for suffixes on your prescription label such as ER (Extended Release), XR (Extended Release), SR (Sustained Release), CR (Controlled Release), LA (Long Acting), CD (Controlled Delivery), XL (Extended Length), or SA (Sustained Action). Any tablet bearing these abbreviations uses a controlled-release mechanism and should be assumed non-crushable. Also watch for EC (Enteric Coated) designations. When in doubt, ask your pharmacist to check the ISMP do-not-crush list for your specific medication.
4. What alternatives exist if you cannot swallow extended release tablets?
Several safer alternatives exist for patients who cannot swallow ER tablets whole. These include liquid or suspension formulations of the same drug, immediate-release versions given at more frequent intervals, transdermal patches, sublingual tablets that dissolve under the tongue, suppository forms, and custom compounded preparations from a compounding pharmacy. Some ER capsules can also be opened and their coated pellets sprinkled on soft food without chewing. OEM/ODM supplement manufacturers like ZhuFeng also offer health products in multiple formats including oral liquids, gummies, and powders for consumers who struggle with tablets.
5. Is crushing a pill the same as splitting it in half?
No, but both compromise the extended-release mechanism. Crushing causes complete destruction, exposing maximum surface area and releasing the entire dose immediately. Splitting exposes the internal matrix at the break point, causing partially accelerated release that is unpredictable. Chewing falls somewhere between the two depending on thoroughness. For osmotic pump tablets like some nifedipine ER products, even splitting is catastrophic because the system depends on an intact membrane. None of these alterations are safe for ER formulations without pharmacist approval.


