

What Is an Extended Release Tablet and Why It Matters
You pick up a new prescription from the pharmacy, glance at the label, and spot two small letters after the drug name: ER. What does ER mean on your medication, and should you take it any differently? If that question has ever crossed your mind, you are far from alone.
An extended release tablet is a dosage form engineered to release its active ingredient gradually over a prolonged period — typically 12 to 24 hours — so that fewer daily doses are needed while maintaining steadier drug levels in the bloodstream.
That single design choice changes almost everything about the way a medication behaves inside your body. Instead of a rapid spike followed by a steep drop, extended release formulations create a smoother, more sustained curve of drug concentration. The result is fewer peaks and troughs, which often translates to reduced side effects and more consistent symptom control throughout the day.
What the Label Actually Means
When you see "ER" on a prescription bottle, the er meaning is straightforward: the tablet (or capsule) has been specially formulated to dissolve slowly rather than all at once. The term applies to both tablets and capsules, and the er definition stays the same regardless of the drug inside. Some manufacturers print "XR" or "XL" instead, but the core concept is identical — a controlled, gradual release of medication over an extended window of time.
Why Extended Release Formulations Exist
Not every drug needs this technology. Extended release formulations exist primarily for medications with short half-lives that would otherwise require dosing every four to six hours, or for drugs where a sudden blood-level spike triggers unwanted side effects. By stretching delivery across the day, these formulations improve convenience, support better adherence, and keep the active ingredient within its therapeutic window — the concentration range where the drug works effectively without causing harm.
In the sections ahead, you will learn exactly how these tablets work at a mechanical level, decode every modified-release abbreviation you might encounter on a label, compare ER to immediate release and delayed release forms, explore which medications commonly use this technology, and — critically — understand why you should never crush, split, or chew an extended release tablet unless explicitly told otherwise.
Every Modified-Release Abbreviation Explained
Prescription labels can feel like alphabet soup. You already know what ER means, but what about XR, SR, CR, or LA printed after a drug name? Each extended release abbreviation signals a specific approach to how your medication dissolves and enters your bloodstream. The table below decodes every common suffix you are likely to find on a pharmacy label or printout — bookmark it for quick reference.
Decoding ER, XR, SR, CR, and Other Suffixes
| Abbreviation | Full Term | What It Means | Brand-Name Example |
|---|---|---|---|
| ER | Extended Release | Drug is released gradually over 12–24 hours, reducing dosing frequency | Metformin ER (Glucophage XR) |
| XR | Extended Release | Same concept as ER — slow, prolonged release throughout the day | Effexor XR (venlafaxine) |
| XL | Extended Length | Designed for once-daily dosing with a steady drug release profile | Wellbutrin XL (bupropion) |
| SR | Sustained Release | Prolongs the drug's release so fewer doses are needed; levels may still fluctuate slightly | Wellbutrin SR (bupropion) |
| CR | Controlled Release | Releases medication at a precise, constant rate to maintain steady blood levels | Ambien CR (zolpidem) |
| DR | Delayed Release | Resists dissolving until it reaches a specific GI location (e.g., intestines), then releases contents | Azulfidine EN-tabs (sulfasalazine) |
| TR | Timed Release | Releases drug in pre-set intervals or after a specific delay period | Chlor-Trimeton TR (chlorpheniramine) |
| LA | Long Acting | Maintains therapeutic effect for an extended duration, often 12–24 hours | Inderal LA (propranolol) |
| CD | Controlled Delivery | Uses a specialized delivery system to control the rate and location of drug release | Cardizem CD (diltiazem) |
| SA / IR | Short Acting / Immediate Release | Drug dissolves quickly and delivers the full dose at once for rapid effect | Ambien (zolpidem IR) |
When you see the sr medical abbreviation on a bottle of bupropion, for instance, it tells you the pill is engineered to sustain medication delivery over several hours rather than releasing everything immediately. Similarly, the xr medical abbreviation on a label of venlafaxine signals you only need one dose per day instead of two or three.
When Abbreviations Overlap in Meaning
Here is where things get confusing: ER, XR, and XL are often used interchangeably by different manufacturers to describe the same fundamental concept — a tablet or capsule that releases its drug slowly over time. The medical abbreviation XR on one brand may be functionally identical to the xl abbreviation medical professionals see on another. Bupropion is a perfect illustration: Wellbutrin SR, Wellbutrin XL, and generic bupropion ER all deliver the same active ingredient through slightly different extended-release mechanisms, yet each label uses a different suffix.
The abbreviation that truly stands apart is DR (delayed release). Unlike ER or SR, delayed release does not mean the drug trickles out slowly. Instead, an enteric coating prevents dissolution until the tablet reaches a targeted section of the GI tract — typically the small intestine — and then it releases its contents all at once. Enteric-coated aspirin is a classic example: the goal is to protect the stomach lining, not to extend the drug's duration of action.
Meanwhile, SA and IR both refer to standard immediate-release forms — the baseline against which every modified-release technology is compared. If you spot an extended release medical abbreviation like ER on your prescription and a friend's bottle shows S/R or XR, the practical takeaway is the same: swallow the tablet whole, follow your prescribed schedule, and never assume you can switch between these suffixes without consulting your pharmacist.
Understanding what these letters mean on your prescription label is one thing — understanding what is actually happening inside the tablet as it travels through your digestive system is another matter entirely.
How Extended Release Tablets Work Inside Your Body
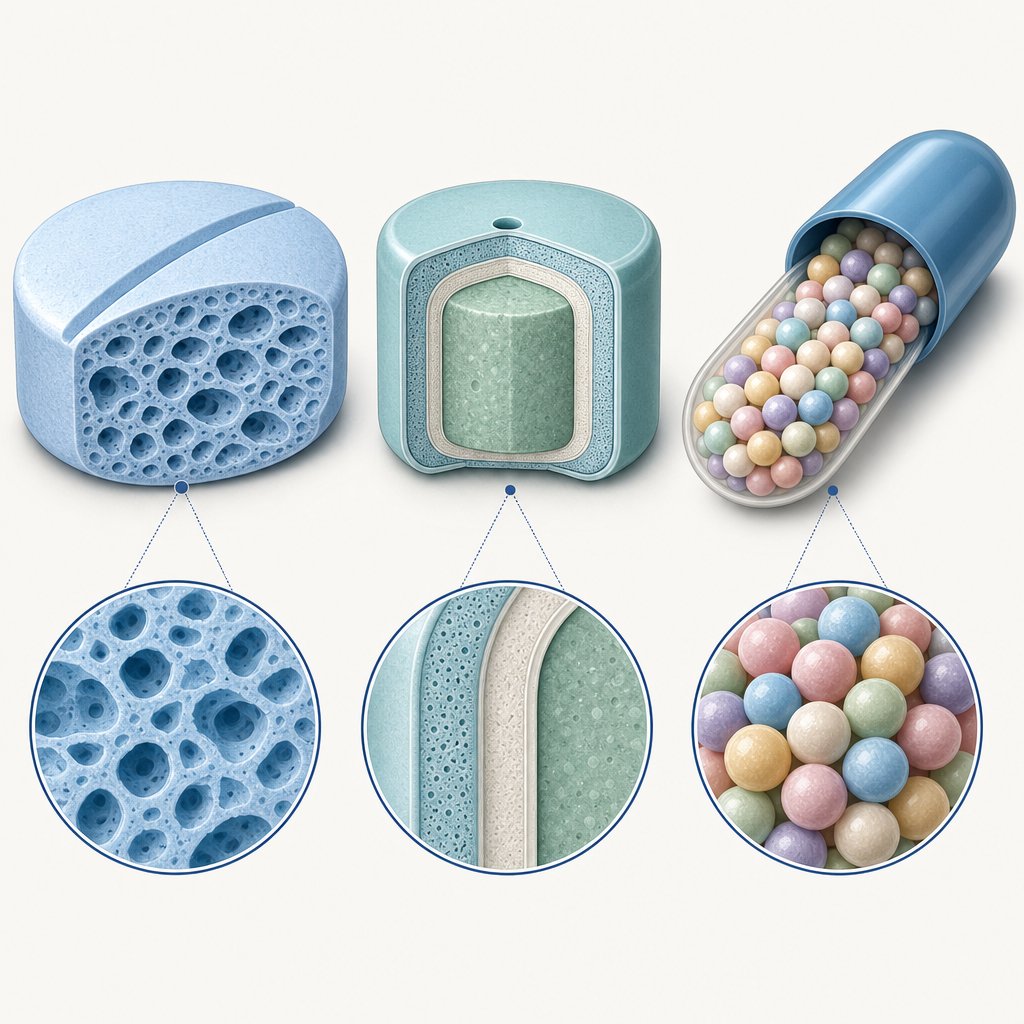
When you swallow an extended release tablet, something far more sophisticated than simple dissolving takes place. The pill enters your gastrointestinal tract and begins interacting with stomach and intestinal fluids in a carefully choreographed process that can span 12 to 24 hours. So how do extended release tablets work at a physical level? Three primary technologies make this possible — and each one uses a different engineering trick to control the time of release.
- Matrix systems — the drug is embedded in a polymer framework that slowly erodes or swells, letting the active ingredient seep out gradually.
- Osmotic pump systems — water is drawn through a semi-permeable membrane by osmotic pressure, pushing a drug solution out through a tiny laser-drilled hole.
- Coated bead and pellet systems — hundreds of tiny drug-loaded pellets with coatings of varying thickness dissolve at staggered intervals inside a single capsule.
Each approach answers the same question — how does extended release work? — but through a very different mechanism. Let's walk through them one at a time.
Matrix Systems and How They Erode
Imagine pressing a drug into a block of sponge-like material. That is essentially what a matrix tablet is: the active ingredient is mixed with a water-swellable polymer — most commonly hydroxypropyl methylcellulose or polyethylene oxide — and compressed into a single solid tablet. When the tablet reaches your stomach and intestinal fluids, the polymer on the outer surface begins to absorb water and swell, forming a thick gel layer.
This gel acts like a gatekeeper. Drug molecules trapped inside must slowly diffuse through a tortuous network of tiny channels within the swollen polymer before they can reach the surrounding fluid and be absorbed. At the same time, the outer gel layer gradually erodes, exposing fresh layers of drug-loaded polymer beneath it. The combination of diffusion through the gel and erosion of the gel surface is what controls how do slow release tablets work in this design.
Pharmaceutical scientists can speed up or slow down release by adjusting two key variables: the type of polymer used and its concentration in the tablet. A higher polymer concentration creates a denser gel with fewer pathways for the drug to escape, which slows the release rate. A lower concentration does the opposite. This flexibility is one reason matrix systems remain the most widely used extended drug release technology on the market — they rely on standard tabletting equipment and safe, well-established excipients.
One trade-off worth noting: because the gel layer interacts with whatever else is in your gut, high-fat meals or variable fluid levels can sometimes alter how quickly the drug is released. This is why some matrix-based ER medications come with specific instructions about taking them with or without food.
Osmotic Pump Technology
If matrix systems work like a slow-eroding sponge, osmotic pump tablets work more like a tiny hydraulic engine. The concept — known as OROS (osmotic-controlled release oral delivery system) — is elegant in its simplicity, even though the engineering behind it is anything but simple.
Here is how does extended release pills work in an osmotic design, step by step:
- The drug is compressed into a tablet core along with an osmotic agent — a substance like sodium chloride or mannitol that strongly attracts water.
- The entire core is coated with a semi-permeable membrane, typically made from cellulose acetate. This membrane allows water molecules to pass through but blocks the drug from leaking out.
- A tiny hole — usually between 0.6 mm and 1 mm in diameter — is drilled through the coating using a precision laser.
- After you swallow the tablet, gastrointestinal fluid passes through the membrane by osmosis, drawn inward by the high osmotic pressure of the core ingredients.
- As water enters, it dissolves the drug and builds hydrostatic pressure inside the tablet. That pressure steadily pushes a solution (or suspension) of the drug out through the laser-drilled orifice at a controlled, predictable rate.
The beauty of this system is its independence from external conditions. Unlike matrix tablets, the drug release rate from an osmotic pump is largely unaffected by the pH or motility of your digestive tract. The rate depends almost entirely on the membrane's permeability and the osmotic pressure gradient — factors locked in during manufacturing. This makes osmotic systems particularly reliable for drugs where even small fluctuations in blood levels can cause problems.
A more advanced version, the push-pull osmotic pump, adds a second layer. One layer contains the drug; the other contains a swelling agent. As water enters, the swelling layer expands and physically pushes the drug layer out through the delivery port — much like squeezing toothpaste from a tube. This design can handle poorly water-soluble drugs that a basic osmotic pump cannot.
Coated Bead and Pellet Systems
Not all extended release products are monolithic tablets. Open certain ER capsules and you will find hundreds of tiny pellets, sometimes called beads or micro-granules, each one loaded with a small amount of the active ingredient. What makes this system work is the coating on each pellet.
Different pellets within the same capsule receive coatings of varying thickness. Thin-coated pellets dissolve relatively quickly after swallowing, releasing their drug payload within the first hour or two. Medium-coated pellets take longer. Thick-coated pellets may not release their contents for six to eight hours. The result is a staggered, wave-like pattern of drug delivery that sustains therapeutic levels over many hours — all from a single capsule taken once or twice a day.
This multiple-unit design offers a practical safety advantage over single-unit tablets. If one pellet's coating fails prematurely, only a tiny fraction of the total dose is released early. With a monolithic tablet, a coating failure could dump the entire dose at once. Pellet systems also tend to empty from the stomach more predictably than large tablets, reducing the risk of being trapped alongside food for prolonged periods.
Why Steady Blood Levels Matter
All three technologies share one overarching pharmacokinetic goal: keeping the drug's concentration in your blood within what pharmacologists call the therapeutic window. This is the range between the minimum effective concentration — below which the drug stops working — and the maximum safe concentration — above which side effects become likely.
When you take an immediate release tablet, blood levels spike quickly to a peak (known as the peak plasma concentration, or Cmax), then decline as your body metabolizes the drug. If that peak overshoots the upper boundary, you may experience dose-related side effects. If levels dip too low before the next dose, symptoms can break through. Extended release formulations flatten that rollercoaster into a gentler plateau. Over multiple doses, blood concentrations settle into what is called a steady state — a consistent level that stays comfortably inside the therapeutic window with minimal fluctuation.
This smoother profile is exactly why physicians prescribe ER formulations for conditions that demand around-the-clock coverage, from chronic pain and high blood pressure to ADHD and depression. The mechanism inside the tablet may differ, but the clinical outcome is the same: more consistent relief with fewer daily doses.
Of course, understanding how these tablets deliver medication is only half the picture. Patients frequently encounter multiple labels — ER, IR, SR, DR — and struggle to grasp how each one actually differs in practice.
Extended Release vs Immediate Release vs Delayed Release
Three letters on a pill bottle — ER, IR, or DR — determine how your medication behaves from the moment it hits your stomach to the moment it leaves your bloodstream. These are not interchangeable labels. Each one describes a fundamentally different release strategy, and confusing them can lead to missed doses, unexpected side effects, or worse. Let's break down each comparison so the differences are impossible to miss.
Extended Release vs Immediate Release
So what is immediate release, exactly? The immediate release definition is straightforward: an IR tablet or capsule dissolves shortly after you swallow it, delivering its full dose into your system as quickly as the drug's chemistry allows. There is no engineered delay, no polymer barrier, and no coating designed to slow things down. The drug races to its peak blood concentration — sometimes within 30 minutes to two hours — and then declines as your body metabolizes and eliminates it.
When you compare extended release vs immediate release on a graph of blood concentration over time, the visual contrast is striking. The IR curve looks like a sharp mountain peak: a steep climb, a narrow summit, and a rapid descent. The ER curve, by contrast, resembles a gently rolling plateau — lower at its highest point, but sustained across many more hours. A pharmacokinetic study of fluvastatin illustrates this vividly: the ER tablet's peak concentration was roughly 78–83% lower than the IR capsule's peak, yet both formulations produced comparable cholesterol reductions over seven days. The ER form achieved similar clinical results while dramatically flattening the blood-level spike.
What does that mean in everyday terms? With an immediate release tablet, you may need to dose two, three, or even four times a day to keep drug levels above the minimum effective threshold. Each dose produces a fresh peak — and each peak carries a risk of dose-related side effects like nausea, dizziness, or headache. ER tablets reduce that rollercoaster to one or two doses daily, keeping blood levels inside the therapeutic window with far less fluctuation.
There is a trade-off, though. Because IR tablets deliver their payload all at once, physicians can titrate doses in smaller, more precise increments. If a patient needs a quick adjustment — say, stepping down from 30 mg to 20 mg — IR forms usually offer more available strengths. ER tablets, by design, are harder to fine-tune and cannot be split to create custom doses without destroying the release mechanism.
Sustained Release vs Extended Release
If you have ever compared labels and wondered whether sustained release vs extended release actually describes two different things, you are asking one of pharmacy's most common questions. The short answer: in most clinical contexts, these terms are functionally synonymous. Both refer to a formulation engineered to slow down drug delivery so that fewer daily doses are needed.
Where some pharmacologists draw a subtle line is in release kinetics. A sustained release (SR) product prolongs the drug's availability but does not guarantee a perfectly constant rate — blood levels may still rise and dip modestly between doses. A controlled release (CR) product, by contrast, aims for a near-constant delivery rate and more uniform blood concentrations. Extended release (ER) serves as the broad umbrella term that covers both approaches. In practice, whether your bottle says SR, ER, XR, or CR, the core instruction remains the same: swallow the tablet whole, do not crush or chew, and follow your prescribed dosing schedule.
Delayed Release vs Extended Release
This is the pair that trips up patients and caregivers most often — and the distinction genuinely matters. Delayed release vs extended release sounds like a difference in speed, but it is actually a difference in location.
A delayed release (DR) tablet is coated with an enteric film that resists dissolving in the acidic environment of the stomach. The coating stays intact until the tablet passes into the more alkaline environment of the small intestine — or sometimes even the colon. Once it arrives at that target location, the coating breaks down and the drug is released all at once, not gradually. Enteric-coated aspirin and sulfasalazine DR are classic examples: the goal is to protect the stomach lining or to deliver medication directly to an inflamed section of the bowel, not to stretch out the drug's duration of action.
An ER tablet, on the other hand, does not care much about where it releases — it cares about how slowly. Drug delivery begins relatively early in the digestive journey and continues over many hours, regardless of GI location. This is why the comparison of delayed release vs extended release is so important: mistaking one for the other could lead you to expect all-day coverage from a DR tablet that was never designed to provide it, or to assume a DR mechanism when your ER tablet's sustained plateau is the actual therapeutic strategy.
The table below puts all three formulation types side by side so you can see the differences at a glance:
| Feature | Immediate Release (IR) | Extended Release (ER / SR) | Delayed Release (DR) |
|---|---|---|---|
| Release Pattern | Full dose dissolves and absorbs rapidly | Drug releases gradually over 12–24 hours | No release until tablet reaches a specific GI location, then releases all at once |
| Dosing Frequency | 2–4 times per day (varies by drug) | Once or twice daily | Varies — often once or twice daily, but timing depends on GI transit |
| Common Use Cases | Acute pain, breakthrough symptoms, dose titration | Chronic conditions requiring around-the-clock coverage (hypertension, ADHD, depression) | Stomach-sensitive drugs, medications targeting the intestines or colon (e.g., ulcerative colitis treatments) |
| Key Abbreviations | IR, SA | ER, XR, XL, SR, CR, LA | DR, EC (enteric coated) |
Think of it this way: immediate release is the default — fast in, fast out. Extended release is about pacing — stretching one dose across many hours. Delayed release is about placement — shielding the drug until it arrives exactly where it needs to go, then letting it loose all at once.
Knowing which type sits inside your pill bottle is the first step. The next logical question is: which medications actually use these formulations — and why was your specific prescription designed as an ER tablet in the first place?

Which Medications Use Extended Release Formulations
Your medication was designed as an ER tablet for a very specific reason — and that reason depends almost entirely on the therapeutic category it belongs to. Some drugs need around-the-clock blood levels to manage chronic symptoms. Others benefit from gentler peaks to avoid dose-related side effects. And a growing number of er medications use extended release engineering as a deliberate barrier against misuse. Here is a practical overview of the major categories where you are most likely to encounter sustained release medication or time release medication on your prescription label.
- Pain management — Extended release pain medication provides continuous relief for chronic conditions such as neuropathic pain, fibromyalgia, and post-surgical recovery, reducing the need for repeated dosing every four to six hours.
- Cardiovascular health — Blood pressure and heart rhythm medications rely on ER formulations to prevent dangerous gaps in coverage that could trigger angina episodes, arrhythmias, or hypertensive spikes overnight.
- Psychiatry and mood disorders — Antidepressants and antianxiety drugs use ER delivery to maintain stable neurotransmitter modulation throughout the day, minimizing symptom breakthrough and withdrawal-like dips between doses.
- ADHD treatment — Stimulant and non-stimulant ADHD medications are formulated as ER to carry children and adults through a full school or work day on a single morning dose, eliminating the stigma and inconvenience of a midday pill.
- Metabolic and diabetes care — Drugs like metformin ER help manage blood sugar steadily while reducing the gastrointestinal side effects — nausea, cramping, diarrhea — that the immediate release version is notorious for.
- Respiratory and allergy relief — Over-the-counter products like guaifenesin ER (Mucinex) use bilayer tablet technology to deliver fast initial relief plus hours of sustained symptom control from a single dose.
Pain Management and Cardiovascular Medications
Chronic pain is one of the oldest and most compelling use cases for extended release medication. When a patient needs relief that lasts through the night or across a full workday, an ER formulation avoids the cycle of dosing, relief, decline, and re-dosing that standard tablets demand. You may have noticed the Tylenol ER pill on pharmacy shelves — so what is Tylenol ER? It is an over-the-counter acetaminophen tablet engineered to release its 650 mg dose gradually over eight hours, intended for minor arthritis and muscle aches that benefit from longer-lasting coverage without increasing the total daily acetaminophen load.
Cardiovascular drugs tell a similar story. Medications like verapamil, metoprolol, and diltiazem must keep blood levels stable around the clock because blood pressure naturally fluctuates — dipping during sleep and surging in the early morning hours. Patients sometimes wonder about verapamil SR vs ER: in practice, both suffixes describe a slow-release formulation of the same calcium channel blocker. The SR version typically requires twice-daily dosing, while some ER or XL versions achieve true once-daily convenience. Either way, the sustained delivery prevents the dangerous gaps that could leave a patient unprotected during a critical window, such as the early morning surge linked to heart attacks and strokes.
Psychiatric, ADHD, and Metabolic Medications
Mental health treatment is where extended release technology arguably makes the biggest quality-of-life difference. Antidepressants like venlafaxine XR and bupropion XL maintain consistent serotonin or dopamine modulation, helping patients avoid the emotional dips and discontinuation-like symptoms that can occur when drug levels fluctuate between immediate release doses. For ADHD, medications such as dextromethorphan/bupropion ER and methylphenidate ER allow a single morning capsule to cover an entire school or workday — a meaningful advantage for both children who would otherwise need a nurse's office visit and adults managing busy schedules.
In diabetes care, metformin ER is one of the most widely prescribed extended release medications in the world. The gradual release profile reduces the gastrointestinal distress that causes many patients to abandon standard metformin, directly improving long-term adherence and blood sugar outcomes.
The Abuse-Deterrent Angle
Beyond clinical convenience, certain ER formulations serve a critical public health function. Opioid painkillers like OxyContin and Hysingla ER, along with specific stimulant medications, are engineered with abuse-deterrent formulations (ADFs) that resist crushing, dissolving, or chemical extraction. These physical and chemical barriers make the tablets far harder to snort or inject — two common routes of misuse that bypass the slow-release mechanism and deliver a dangerously concentrated dose all at once. The FDA has approved abuse-deterrent labeling for products including OxyContin, Hysingla ER, Xtampza ER, and RoxyBond, and continues to encourage the conversion of the opioid market toward these safer designs. It is important to understand that abuse-deterrent does not mean abuse-proof — swallowing the intact tablet can still carry addiction risk — but the technology represents a meaningful step in reducing the most dangerous forms of prescription drug misuse.
With so many therapeutic categories relying on this technology, the natural follow-up question is whether the benefits always outweigh the trade-offs — and where ER formulations genuinely fall short.
Benefits and Limitations of Extended Release Tablets
Every medication format involves a compromise. Extended release tablets deliver undeniable advantages for millions of patients managing chronic conditions — but they also carry a specific set of drawbacks that rarely make it into the conversation. Understanding both sides helps you make informed decisions alongside your prescriber rather than discovering limitations the hard way.
Key Benefits of Extended Release Dosing
The clinical case for extended-release tablets rests on a pharmacokinetic principle you already understand from earlier sections: smoother blood levels mean fewer side-effect spikes and more consistent symptom control. Here is how that translates into real-world advantages:
- Fewer daily doses improve adherence. A study of over 123,000 patients across 15 chronic medications found that XR users had an average adjusted medication possession ratio of 80.2%, compared with 74.8% for non-XR users — a 5.4% improvement that is clinically meaningful. Adjusted adherence rates were even more striking: 56.3% for XR users versus 46.0% for non-XR users.
- Steadier blood levels reduce peak-related adverse effects. Many dose-dependent side effects — dizziness, nausea, flushing — are triggered by the rapid concentration spike that follows an immediate release dose. Extended release pills flatten that spike, keeping levels within the therapeutic window and minimizing discomfort.
- Overnight and all-day symptom coverage. Conditions like hypertension, chronic pain, and depression do not take breaks. A single ER dose at bedtime or in the morning can provide uninterrupted protection through the hours when patients are asleep or too busy to remember a midday pill.
- Reduced peak-to-trough fluctuations. Less swinging between "too much drug" and "not enough drug" means the active ingredient spends more total time inside its effective range, which can translate to better clinical outcomes over weeks and months.
- Lower abuse potential for certain formulations. As noted in the previous section, time release pills engineered with abuse-deterrent features resist the crushing and extraction techniques most commonly associated with prescription drug misuse.
Taken together, these benefits explain why extended-release tablets have become a cornerstone of chronic disease management. Yet the same engineering that creates these advantages introduces a distinct set of trade-offs that patients and caregivers deserve to know about.
Limitations and Drawbacks to Consider
No prescriber or pharmacist should present ER formulations as universally superior. In certain clinical scenarios, the standard immediate release tablet is actually the better tool. Here are the limitations worth weighing:
- Less dosing flexibility during titration. The same property that smooths out drug delivery also means ER tablets cannot be adjusted in small increments the way IR tablets can. If a physician wants to move a patient from 15 mg to 20 mg, an IR product may offer both strengths, while the ER equivalent might only come in 15 mg and 30 mg options. Fine-tuning becomes harder.
- Difficulty swallowing larger tablets. Because ER formulations must house both the active ingredient and the polymer matrix, osmotic shell, or pellet system that controls release, the tablets tend to be physically larger than their IR counterparts. For elderly patients or anyone with dysphagia or GI narrowing, this size difference can be a genuine barrier to compliance.
- Generally higher cost. Manufacturing specialized coatings, osmotic membranes, and multi-layered pellet systems adds expense. Research involving 15 chronic medications found that average out-of-pocket costs for a 30-day supply were $7.46 higher for XR formulations — and that cost difference was strongly correlated with lower XR adoption rates. When a generic immediate release version costs hundreds of dollars less, the clinical advantage of ER must be weighed against the financial burden on the patient.
- Inability to split or crush without destroying the release mechanism. This is perhaps the most critical practical limitation. Cutting, chewing, or grinding an extended release tablet can bypass hours of carefully engineered delivery, potentially releasing the entire dose at once. The consequences range from intensified side effects to life-threatening overdose.
- Slower onset when rapid relief is needed. Extended release formulations are designed for sustained control, not for acute symptom management. If a patient needs fast-acting pain relief after an injury or immediate anxiety reduction during a panic attack, an ER product is the wrong choice. Fentanyl patches illustrate this point clearly: their very slow onset makes them inappropriate for acute pain, despite being highly effective for chronic, around-the-clock management.
- Prolonged side effects when they do occur. The flip side of long-lasting therapeutic coverage is long-lasting adverse effects. If a patient develops a troublesome reaction to an ER product, that reaction may persist for many more hours than it would with a short-acting formulation. A weekly extended release injection like exenatide (Bydureon) makes this trade-off especially stark — any side effect lingers far longer than it would with the twice-daily IR version (Byetta).
The "Ghost Tablet" — Why Your Pill May Appear in the Toilet
Imagine glancing into the toilet after a bowel movement and seeing what looks like an intact tablet sitting there. Your first instinct might be panic: did my body just pass the medication without absorbing it?
This phenomenon — widely known as the ghost tablet or ghost pill — is one of the most common yet least discussed concerns among patients taking extended-release tablets. And it is almost always harmless. In matrix-based and osmotic pump designs, the outer shell or polymer framework is inert. It was never meant to dissolve. Its only job was to house the active drug and control its release rate as the tablet traveled through your digestive tract. By the time the empty shell reaches the colon, the medication has already been absorbed into your bloodstream.
Clinical case reports paint a vivid picture of the anxiety this can cause. One published case describes a 65-year-old man taking OxyContin who became convinced his pain medication was passing through unabsorbed after he noticed round tablet-like objects in his stool. His pain specialist was equally puzzled. In another case, a 69-year-old woman taking venlafaxine XL collected ghost pills from her stool and brought them to her doctor — only to find that multiple healthcare professionals she had told did not understand the phenomenon either. Her medication was unnecessarily switched back to the immediate release formulation, which ultimately led to a psychiatric hospitalization for persistent symptoms.
The prescribing information for many osmotic and matrix ER products explicitly warns about this. The OxyContin label, for example, states that patients "may pass empty matrix 'ghosts' via colostomy or in the stool" and reassures that "the active medication has already been absorbed." Similar language appears in patient leaflets for Concerta (methylphenidate OROS), Pristiq (desvenlafaxine), and Wellbutrin XL (bupropion). If you notice what looks like an intact tablet in your stool and you are taking any of these extended-release tablets, there is almost certainly no reason for alarm. The drug did its job — the shell is simply what is left over.
That said, if ghost tablets appear alongside unexplained symptom worsening — increased pain, returning depression, or breakthrough seizures — contact your prescriber. Conditions that speed up GI transit, such as severe diarrhea or short bowel syndrome, can occasionally push an ER tablet through the system before it has fully released its contents. In these situations, the ghost pill is not just cosmetic — it may signal incomplete absorption that needs clinical attention.
Both the benefits and the limitations above share a common thread: they all trace back to the engineered release mechanism inside the tablet. Disrupt that mechanism — whether by crushing, splitting, mixing with alcohol, or skipping doses — and the carefully balanced pharmacokinetic profile collapses. The safety risks that follow deserve their own detailed discussion.

Safety Risks and What to Avoid With ER Tablets
The engineering inside an extended release tab is precise, deliberate, and surprisingly fragile. Every polymer layer, every osmotic membrane, every pellet coating was calibrated to deliver a specific amount of drug over a specific number of hours. Remove that structure — by crushing, chewing, splitting, or mixing with the wrong substance — and the entire pharmacokinetic contract between the tablet and your body breaks down. The consequences range from uncomfortable to life-threatening. This section covers the three safety domains that matter most: dose dumping, missed-dose management, and food and substance interactions that can silently alter how ER tablets and ER pills behave.
What Is Dose Dumping and Why It Is Dangerous
Imagine taking a medication designed to deliver its contents over 12 hours — and receiving the entire dose in 15 minutes instead. That scenario has a clinical name: dose dumping. It occurs when the release mechanism of an ER tablet is compromised, causing the full payload of active ingredient to flood the bloodstream all at once.
The most common cause is mechanical destruction. Crushing, splitting, or chewing an extended release tablet physically shatters the matrix, membrane, or coating that controls delivery. A clinical resource from Enclara Pharmacia warns that manipulating modified-release formulations — including ER, XR, XL, SR, CR, and LA products — "may alter the release mechanism, potentially leading to dose dumping and increased toxicity." The risk is not theoretical. ER opioids like morphine sulfate extended release (MS Contin) can contain doses of 60 mg or more in a single tablet — an amount intended to trickle into the bloodstream over half a day. Release that dose instantaneously, and blood concentrations can spike to overdose levels, causing respiratory depression, sedation, or death.
The danger extends beyond opioids. Cardiovascular ER medications crushed before administration can trigger sudden blood pressure drops. Stimulant ER formulations for ADHD, if chewed, can deliver a jolt of medication that causes tachycardia and agitation. Even something as routine as an extended release potassium chloride tablet, if crushed, can cause severe gastrointestinal ulceration from the concentrated salt hitting a single spot on the mucosal lining.
What should you do if you accidentally chew or crush an ER tablet? Contact your pharmacist or poison control immediately — do not wait for symptoms to appear. Time matters because the window for intervention narrows rapidly once the full dose enters the bloodstream. For anyone wondering what does ER mean in medical terms, this risk alone captures why those two letters carry such weight: they signal a formulation that must remain structurally intact to function safely.
Never crush, split, or chew an extended-release tablet unless the prescribing information explicitly says it is safe to do so. Destroying the release mechanism can deliver the entire dose at once, creating potentially life-threatening drug concentrations.
Missed Doses and Timing Considerations
You glance at the clock and realize your morning ER dose was supposed to be taken three hours ago. Should you take it now? Double up at the next scheduled time? Skip it entirely? The answer depends on several factors — the specific medication, how late you are, and how frequently you dose — but a few universal principles apply to virtually every extended release means of delivery.
General guidance from the NHS Specialist Pharmacy Service breaks the decision into two scenarios:
- Dose less than two hours late: For most medications, it is acceptable to take the dose and continue your regular schedule. You may notice slightly increased side effects if the interval before the next dose becomes shorter than usual.
- Dose more than two hours late: If you take the medication once or twice daily, take the missed dose as soon as you remember — provided the next dose is not due within a few hours. If it is, skip the missed one. For medications dosed more than twice daily, simply skip the missed dose and resume at the next scheduled time.
One rule overrides everything else: never take a double dose to make up for a forgotten one. ER formulations already contain a larger quantity of drug than their immediate release equivalents — doubling up could push blood concentrations far above the safe ceiling, essentially creating a voluntary dose dump.
Certain medications carry higher stakes when a dose is missed. Antiseizure drugs like levetiracetam, for example, require consistent blood levels to prevent breakthrough seizures. The Epilepsy Society recommends that for twice-daily medicines, a forgotten dose can be taken if it is within six hours of the scheduled time. Beyond that window, skip it. Parkinson's disease medications are even more time-sensitive — a delay of just 30 minutes can worsen motor symptoms significantly, and abrupt missed doses carry a risk of neuroleptic malignant syndrome.
The bottom line: specific rules vary by medication. Your patient information leaflet — the folded paper insert inside every prescription box — contains tailored missed-dose instructions. When in doubt, call your pharmacist before improvising.
Food and Substance Interactions
What you eat or drink alongside an ER tablet can quietly alter how much drug reaches your bloodstream and how quickly it gets there. Two interactions deserve particular attention: alcohol and high-fat meals.
Alcohol is the more dangerous variable. A clinical pharmacokinetic study published in Clinical Pharmacology: Advances and Applications tested the effect of alcohol on extended-release hydrocodone in healthy volunteers. When HC-ER was taken with a 20% alcohol solution (roughly equivalent to three shots of vodka), systemic exposure remained largely unchanged. But at 40% alcohol concentration — equivalent to five or six shots on an empty stomach — the results were alarming: peak blood concentration of hydrocodone spiked approximately 2.3-fold higher than without alcohol, and time to peak was cut in half (2.43 hours versus 6.16 hours). Among individual subjects, the maximum increase in peak concentration reached 3.9-fold. Adverse events jumped from 10% of subjects at 0% alcohol to 66.7% at 40% alcohol.
The mechanism is straightforward: alcohol can partially dissolve the polymer coatings or matrices that control drug release in certain ER formulations, accelerating the rate at which the active ingredient enters your system. Even when full-blown dose dumping does not occur, the elevated peaks and shortened time to peak effectively turn an extended release tablet into something closer to an immediate release overdose. This interaction is not unique to opioids — researchers have documented similar alcohol-induced acceleration with ER formulations of morphine, oxymorphone, and tapentadol.
High-fat meals introduce a subtler but still clinically relevant effect. Fat slows gastric emptying, which can keep an ER tablet sitting in the stomach longer than intended. For some formulations, this prolongs contact with gastric fluids and increases peak absorption. The same hydrocodone study found that food produced a modest increase in peak concentration (28.86 ng/mL fed versus 22.74 ng/mL fasted) without significantly changing total drug exposure. For other ER products — particularly oxymorphone ER — the food effect is large enough that prescribing information explicitly directs patients to take the medication on an empty stomach, at least one hour before or two hours after eating.
A practical checklist for safe ER tablet use:
- Avoid alcohol entirely while taking ER medications unless your prescriber has confirmed it is safe for your specific drug.
- Read your medication label for food-timing instructions — "take with food" and "take on an empty stomach" are not interchangeable, and the wrong choice can alter your drug levels meaningfully.
- Grapefruit and grapefruit juice inhibit enzymes that metabolize many ER drugs, potentially raising blood concentrations. Check your patient leaflet for warnings.
- If you experience unusual drowsiness, dizziness, or a sudden intensification of side effects after eating a heavy meal or consuming alcohol with your ER medication, contact your healthcare provider promptly.
Each of these safety risks — dose dumping, missed-dose errors, and food or alcohol interactions — ultimately traces back to the same engineering reality: an ER tablet's release mechanism is a precision instrument. Its therapeutic value depends entirely on that mechanism remaining intact and operating under the conditions it was designed for. Understanding what does ER mean in medical terms goes beyond a simple label definition — it means recognizing that the tablet's structure is inseparable from its safety profile.
That precision engineering also raises an important question from the other side of the equation: how do pharmaceutical companies decide which drugs warrant this level of formulation complexity, and what goes into building these tablets at scale?
How Extended Release Tablets Are Developed and Manufactured
Not every drug ends up inside an extended release shell. Pharmaceutical companies invest in controlled release technology only when the drug's pharmacological profile creates a genuine clinical problem that standard tablets cannot solve. The decision is driven by science, not marketing — and the development process behind sustained release tablets is far more demanding than most patients realize.
Why Some Drugs Need Extended Release Formulations
Picture a drug with a half-life of just three to four hours. If it treats a chronic condition — hypertension, depression, diabetes — patients would need to swallow a pill four, five, or even six times a day to maintain effective blood levels. Missed doses become almost inevitable, and each gap in coverage opens a window for symptom breakthrough. This is the first and most straightforward criterion: drugs with short half-lives that would otherwise require inconveniently frequent dosing are prime candidates for ER formulation.
A second trigger is peak-level toxicity. Some drugs produce troublesome side effects — nausea, dizziness, cardiovascular stress — only when blood concentrations spike above a certain threshold. If the therapeutic dose sits uncomfortably close to that toxicity threshold, flattening the concentration curve with an ER design can preserve efficacy while pulling the peak below the danger line. Metformin is a textbook example: the immediate release version causes GI distress in a significant percentage of patients, while the ER formulation smooths out local drug concentrations in the gut and dramatically reduces those complaints.
The third criterion is patient compliance. Sustained release medications refer to formulations engineered specifically to reduce pill burden in populations where adherence is a documented challenge — psychiatric patients managing bipolar disorder, children with ADHD, elderly patients juggling multiple prescriptions. When missing a single dose carries serious clinical consequences, reducing the daily pill count from three to one is not a convenience — it is a safety measure.
When none of these criteria apply — when a drug already has a long half-life, a wide therapeutic window, and manageable dosing — there is simply no pharmacological justification for the added complexity of an ER format. Drugs like amlodipine (half-life of 30 to 50 hours) work perfectly well as standard tablets because the body already handles their elimination slowly enough to maintain stable blood levels with once-daily dosing.
From Formulation Design to Scalable Production
Deciding that a drug needs extended release is only the beginning. Building the actual tablet — whether it uses a matrix system, an osmotic pump, or a sustained release capsule filled with coated pellets — demands specialized expertise that spans multiple disciplines.
The formulation team must first select the right polymer system. Hydrophilic polymers like hydroxypropyl methylcellulose (HPMC) swell into gels that control diffusion rates. Hydrophobic polymers like ethylcellulose create insoluble barriers. Acrylic polymers such as methacrylic acid copolymers offer pH-dependent release profiles. Each choice shapes the drug's release curve differently, and matching the right polymer to the desired release profile is one of the primary challenges in ER development.
Next comes coating technology. For osmotic systems, a semi-permeable membrane must be applied with exact thickness tolerances — too thin and the drug releases too fast; too thick and patients may not absorb enough. For extended release capsules and time release capsules that rely on multiparticulate pellet systems, each bead requires a precisely calibrated coating layer. Hundreds of pellets inside a single capsule may carry three or four different coating thicknesses to stagger their dissolution times across hours.
Dissolution testing then validates the design. Engineers run in vitro experiments that simulate gastric and intestinal fluid conditions to confirm the tablet releases its drug at the intended rate. When comparing modified release vs sustained release profiles, the dissolution test is where subtle kinetic differences — zero-order versus first-order release — become measurable. These results feed into in vitro-in vivo correlation (IVIVC) models that predict how the tablet will perform inside a real patient, reducing the need for repeated human bioequivalence studies.
Finally, stability studies must demonstrate that the release profile holds up over the product's shelf life — across temperature swings, humidity changes, and extended storage. A tablet that performs perfectly on day one but releases its drug too quickly after six months in a medicine cabinet is a failed product.
This entire development pipeline — polymer selection, coating application, dissolution validation, stability confirmation — requires infrastructure and know-how that many companies simply do not have in-house. Generic drug manufacturers trying to match an innovator's ER product face an especially steep challenge: they must reverse-engineer a release profile and demonstrate bioequivalence without access to the original formulation data.
This is where contract manufacturing plays a critical role. OEM/ODM partners with deep formulation expertise allow brands to bring modified-release and specialized tablet products to market without building costly internal R&D and production capabilities from scratch. For businesses in the health supplement and functional food space — where product format diversity is a competitive advantage — experienced contract manufacturers offer turnkey solutions that cover everything from initial formulation design to large-scale production.
ZhuFeng, for example, provides OEM/ODM health food manufacturing services across a wide range of delivery formats: tablets, hard capsules, soft capsules, powder and granules, gummy candy, and oral liquids. Their customized formulation and scalable production capabilities serve nutrition brands, supplement importers, and private label sellers looking to launch market-ready products — whether the goal is a standard tablet, a specialized capsule design, or an entirely new product concept tailored to a specific consumer segment.
The broader takeaway is practical: the technology behind ER formulations is not limited to Big Pharma labs. Contract manufacturers have made specialized tablet and capsule production accessible to a much wider range of businesses, lowering the barrier between a promising product idea and a finished, market-ready format.
With the science and manufacturing landscape covered, the final piece of the puzzle is equally important — how to take these medications correctly every day and how to choose the right product format for your specific needs.

Practical Tips and Choosing the Right Tablet Format
Everything you have read so far — the mechanisms, the abbreviations, the safety risks, the manufacturing complexity — boils down to a surprisingly simple daily reality: you standing at your kitchen counter with a glass of water and a pill in your hand. Getting that moment right, every single time, is what separates effective treatment from preventable problems. Here are the rules that matter most.
Practical Tips for Taking ER Medications Correctly
- Swallow the tablet whole with a full glass of water. Do not crush, split, or chew it unless your prescribing information explicitly states this is safe. As MD Anderson's pharmacy team emphasizes, medications labeled "extended release," "controlled release," or "delayed release" are specially formulated to deliver a calculated amount of drug over a specific period — breaking the structure can release everything at once, risking organ damage or worse.
- Take your dose at the same time every day. Consistency keeps blood levels inside the therapeutic window. Whether you choose 8 a.m., noon, or bedtime, stick to your schedule. Set a phone alarm if mornings are chaotic.
- Never double up after a missed dose. ER tablets already contain more active ingredient than their immediate release equivalents. Taking two at once effectively creates a voluntary dose dump. If you miss a dose, follow the guidance in your patient information leaflet or call your pharmacist.
- Store your medication properly. Heat, humidity, and direct sunlight can degrade the polymer coatings and matrices that control drug release. Keep ER tablets in their original container at room temperature unless the label specifies refrigeration.
- Do not panic over ghost tablets. If you see what looks like an intact pill in your stool, remember that many matrix and osmotic pump designs leave behind an inert shell after the drug has been fully absorbed. Report it to your prescriber only if your symptoms worsen at the same time.
- Always read the patient information leaflet. That folded paper insert inside your prescription box contains drug-specific instructions about food timing, alcohol warnings, and what to do if you accidentally chew a tablet. Five minutes of reading can prevent hours of avoidable trouble.
If you have ever wondered what is time release pills or whether your specific medication qualifies, these same six rules apply universally. The definition of extended release — a formulation designed to deliver its active ingredient gradually rather than all at once — means the tablet's physical structure is doing critical work that your compliance habits must support.
Choosing the Right Product Format for Your Needs
For patients, the choice between an ER tablet, a capsule, or a standard immediate release form is ultimately a clinical decision made with your prescriber. It depends on the drug's half-life, your tolerance for side effects, your ability to swallow larger tablets, and whether your condition demands around-the-clock coverage or fast-acting relief. Is sustained release same as extended release? In nearly all clinical contexts, yes — both terms describe a formulation that slows drug delivery to reduce dosing frequency. What does delayed release mean? It refers to a different strategy entirely: shielding the drug until it reaches a specific part of your digestive tract, then releasing the full dose at that location. Knowing which type you are taking prevents confusion and keeps you safer.
For businesses developing health supplements, functional foods, or nutraceutical products, the format decision is equally consequential — but the variables shift toward consumer preference, bioavailability targets, and market positioning. Oral dosage form comparisons consistently show that each format carries distinct trade-offs: tablets offer the lowest manufacturing cost and highest dose density, capsules provide superior taste masking and formulation flexibility, gummies drive consumer compliance through palatability, and powders or oral liquids serve populations that cannot swallow solid forms. Matching the right format to your target audience is not a cosmetic decision — it directly affects absorption, shelf stability, and repeat purchase rates.
Experienced OEM/ODM partners can streamline this process considerably. ZhuFeng's health food manufacturing services, for instance, support the full spectrum of delivery formats — tablets, hard capsules, soft capsules, powder and granules, gummy candy, and oral liquids — with customized formulation tailored to each brand's target market. For nutrition brands, supplement importers, and private label sellers exploring what is a time release pill format or any other specialized delivery system, having a manufacturing partner with cross-format expertise means faster development cycles, fewer reformulation dead ends, and a product that reaches shelves ready to compete.
Understanding how your medication releases its active ingredient — whether gradually through an ER matrix, all at once from an IR tablet, or at a targeted location via a DR coating — empowers you to take it more safely, ask sharper questions, and get more consistent results from every dose.
The meaning of extended release is ultimately about control: control over how much drug enters your bloodstream, control over how long it stays there, and control over how your daily routine accommodates the treatment plan your prescriber designed. Respect the tablet's structure, follow the six rules above, and those two small letters on your label — ER — become an ally rather than a mystery.
Frequently Asked Questions About Extended Release Tablets
1. Can you crush or split an extended release tablet?
No. Crushing, splitting, or chewing an ER tablet destroys the built-in release mechanism — a polymer matrix, osmotic membrane, or coated pellet system — that controls how the drug enters your bloodstream over 12 to 24 hours. Breaking that structure can cause dose dumping, where the entire dose floods your system at once. This can lead to dangerously high blood concentrations, severe side effects, or even overdose. Always swallow ER tablets whole with a full glass of water unless your prescribing information or pharmacist explicitly confirms the tablet is safe to split.
2. What is the difference between ER and DR on a prescription label?
ER (extended release) and DR (delayed release) describe two completely different strategies. An ER tablet releases its active ingredient slowly over many hours to maintain steady blood levels and reduce dosing frequency. A DR tablet, by contrast, uses an enteric coating that prevents the pill from dissolving until it reaches a specific part of the gastrointestinal tract — usually the small intestine — and then releases its full dose all at once. DR protects the stomach or targets a specific GI location, while ER controls the pace of delivery over time. Confusing the two can lead to incorrect expectations about how long the medication will remain active.
3. Why does my extended release pill appear whole in my stool?
This is known as a ghost tablet, and it is almost always harmless. Many ER tablets — especially those using matrix or osmotic pump technology — have an inert outer shell that is not designed to dissolve. As the tablet travels through your digestive tract, the drug is gradually absorbed into your bloodstream. By the time the empty shell reaches your colon, the active ingredient has already done its job. Prescribing information for products like OxyContin, Concerta, and Wellbutrin XL specifically warns patients to expect this. However, if ghost tablets appear alongside worsening symptoms such as increased pain or breakthrough seizures, contact your prescriber to rule out incomplete absorption.
4. Is it safe to drink alcohol while taking extended release medication?
Alcohol can be dangerous with ER medications. Clinical studies show that high-concentration alcohol can partially dissolve the polymer coatings that control drug release, accelerating absorption and spiking peak blood levels. In one study of extended-release hydrocodone, 40% alcohol raised peak drug concentration by up to 3.9 times and cut the time to reach that peak in half. This effectively turns a controlled-release tablet into a rapid-release overdose risk. Even moderate alcohol intake may alter the absorption profile of certain ER drugs. Unless your prescriber has confirmed your specific medication is safe with alcohol, it is best to avoid it entirely.
5. What types of medications commonly come in extended release form?
Extended release formulations are widely used across several therapeutic categories. Pain management drugs provide around-the-clock relief without frequent redosing. Cardiovascular medications like verapamil and metoprolol maintain stable blood pressure throughout the day and night. Psychiatric drugs including venlafaxine XR and bupropion XL support consistent neurotransmitter modulation. ADHD stimulants like methylphenidate ER allow a single morning dose to cover a full school or work day. Diabetes medications such as metformin ER reduce GI side effects while managing blood sugar steadily. Even OTC products like guaifenesin ER (Mucinex) use this technology for sustained symptom relief from a single dose.


